Appendix A: Citizens’ Health Care Working Group Community Meetings: Overview of Local Demographics and Health Resources
Appendix B: Summary of Community Meeting Data
Appendix C: Working Group Health Care Poll
Appendix D: University Town Hall Survey
Appendix E: Health Care Presentations
Appendix F: National Health Care Polls and Survey Reports Related to the Working Group Analyses
Appendix G: Public Comments on Interim Recommendations
How We Did Our Work
Hearings
In the summer and early fall of 2005, the Working Group held hearings in Crystal City, Virginia; Jackson, Mississippi; Salt Lake City, Utah; Houston, Texas; Boston, Massachusetts; and Portland, Oregon to learn about the nation’s health care system. At the first hearings, health policy experts provided a common foundation on topics including employer-based and other private insurance, public programs including Medicare and Medicaid, health care costs, and public and private initiatives to control costs and expand insurance coverage. At the subsequent hearings topics included: the uninsured and underserved, health care quality, geographic variation in health care utilization, health information technology, rural health issues, mental health, health care disparities, long-term care, end-of-life care, community-based care, and Oregon’s experience in public engagement on health care issues.
We also heard of many private and public programs trying to expand access to care, improve quality, and reduce costs. Some of the programs we heard about were state and local programs to expand health insurance coverage; employees and employers working together to expand access by holding costs down and getting the right care at a good price; using health care technology to reduce medical errors, monitor patient care, and choose the most appropriate care for patients; providing more information to providers and patients for making choices about health care; encouraging people to use less expensive but equally effective care such as generic drugs; adjusting payments to doctors, hospitals, and other health care providers based on the quality of care they provide; and improving people’s access to care and insurance coverage through more effective use of current programs or new programs that will allow small business and self-employed individuals to obtain coverage.
Many of the programs are new, so we don’t know yet how well they will work over the long term. And, because these programs were designed to work in particular places, we don’t know whether the programs would fit, or work successfully, in other locations or settings. However, the hearings reinforced our conclusion, as stated in the Health Report to the American People, that we need to address the entire health care system, not just specific problems in cost, quality, or access, no matter how urgent they may seem from our different perspectives. Ideally, savings gained from improving efficiency and quality in the system could be used to make other needed changes. Some of the proposed health care initiatives could help to keep the amount and type of some health care services we receive the same, while controlling costs and improving quality. But we also concluded that none of the initiatives that we reviewed could provide all the answers to our health care system’s problems. Rather, the hearings helped lay the groundwork for the search for solutions described in this report.
A complete list and brief description of the 61 presentations made by experts at these hearings is found in Appendix E.
Public Dialogue
The Working Group conducted community meetings throughout the United States to hear from, and begin a dialogue with, the American people. As stated in the statute, these meetings constitute the primary source of input that the Working Group has used in developing its preliminary recommendations. In addition, however, a variety of complementary forms of input (described below) have been important. These different types of input were designed to engage a broad segment of the American public in an informed discussion, using formats that allowed both
-
free expression of all views, and
-
sufficient structure to allow the Working Group to characterize and compare different views in order to reach conclusions based on the dialogue.
Working Group Community Meetings
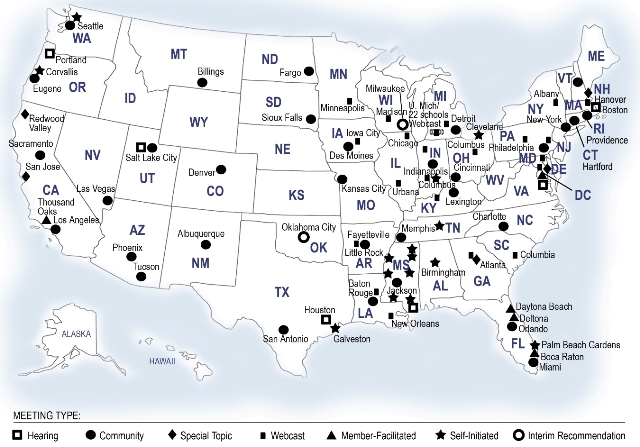
The Working Group conducted 31 Community Meetings in 28 states between January and May 2006 (see Appendix A). These meetings ranged in size from about 35 to approximately 500 participants. At least one Working Group Member attended each meeting. Each meeting was organized using one of a set of formats designed for meetings of different lengths, but all were based on discussion of the four questions to the American people posed in the legislation. The discussion guides, as well as other background materials developed for the meetings (videos, slides, etc.), were all based on the analysis of issues confronting the American health care system presented in the Working Group’s publication, The Health Report to the American People, with some updated facts and figures. Audience generation for the community meetings consisted of outreach through both earned and paid media, involvement of national and local organizations, associations, and other groups, and the participation of various leaders and government officials at the local, state and national levels. Professional meeting facilitators led the meetings.
The basic structure of the meetings involved discussion among participants sitting in small groups, and a structured process for reporting the views of the groups. At the 31 Community Meetings, electronic devices allowed individuals to provide responses to all or some of the same questions included in the poll posted on the Working Group Internet site (see Appendix C), and used in other polls and surveys. The responses to each question were then displayed on a screen, providing immediate feedback to the participants. As discussed in "The Dialogue" (below), there was some variation in the wording of the "standard" questions from meeting to meeting, in response to the preferences of the groups. The format therefore allowed participants to alter the discussion when they felt it was important to do so, while providing enough consistency to allow for comparisons on key issues. Attendees were also encouraged to provide written comments, and many did so. Staff of the Working Group also considered these comments in their review of the meetings.
Additional Meetings
Another important set of discussions took place at the University town hall meeting sponsored by the Big Ten Conference and the Association of Schools of Public Health, and hosted by the University of Michigan on March 22, 2006 (see Appendix D). This virtual town hall provided a forum for individuals gathered at 22 separate public meetings organized by the participating universities, along with the webcast of the meeting from the University of Michigan, as well as people viewing the live webcast across the country. Interactive technology allowed various locations to call in with questions and comments, and individuals submitted their feedback about health care in America through e-mail to be read to participants during the live event.
Still other meetings organized by individual Working Group Members and staff in collaboration with community based health, advocacy, and business groups provided additional insights and opportunities to hear from people with perspectives that might not have been well represented at the other community meetings (see below). Some of these were directly related to issues that were raised in the hearings held by the Working Group (see Appendix E). These special meetings included sessions focusing on mental health, health care at the end of life, chronic illness and disability, a series of meetings in rural areas of Mississippi, a meeting co-hosted with Native American organizations, and a meeting organized by a national association representing realtors.
The Working Group also reviewed data from additional meetings that members as well as other people throughout the country conducted on their own, using materials developed by the Working Group and made available to the public in the "Community Meeting Kit" available on the web site. A listing of meetings that have provided data to the Working Group is included at the end of this section. Other organizations have also provided us with information. Among these are: The National Health Care for the Homeless Council (NHCHC), which conducted a nationwide outreach effort to gather the input of homeless persons; data from the responses of 446 homeless persons in 12 cities were provided to the Working Group.
Other Direct Citizen Input
The Working Group solicited input from people across the country via the Internet, at www.citizenshealthcare.gov, and by mail.
The Working Group Public Comment Center on its web site solicited both structured and unstructured comments from the public.
-
"What’s Important to You" sought responses to four broad questions about people’s concerns about health care in America, views on changing the way health care is delivered or paid for, trade-offs that people would be willing to make to improve health care, and recommendations that people would make to improve health care for all Americans. The responses submitted by over 4,600 people from across the United States were coded into response categories and analyzed. The full text of close to 2,200 hand written responses was also provided to the Working Group for review. The United Church of Christ provided us with about 1,500 hand-written responses from people in about 10 percent of its 5,700 churches across the country to the open-ended questions posted on our Internet site; these are included in our analysis.
-
Close to 600 people wrote to the Working Group, via the CHCWG Internet "Share Your Experience" page or in handwritten letters, to tell us about their own stories. Many of these described problems obtaining or paying for adequate health insurance or quality health care; some described very positive experiences with the health care system.
-
The Health Care Poll posted on the web site drew over 13,000 responses from January through August 31 (see Appendix C). The Catholic Health Association (CHA) also provided over 1,000 poll responses that were submitted directly to CHA’s web site. These are included in the analysis of poll data; the responses are also presented in Appendix C. A number of organizations, including Communication Workers of America (CWA), Starbucks Coffee Company, The National Health Law Program, the National Assembly on School Based Health Care, Wheaton Franciscan HealthCare, and the American Nurses Association also provided information and links to encourage people to provide input to the Working Group. Many people affiliated with these groups participated in community meetings and via the Internet. More than 500 members of the CWA responded to the Internet poll (see Appendix C). Additionally, many of the organizations that conducted their own meetings sent us paper polls. The Area Agency on Aging in Florida provided about 50 poll responses from seniors in Florida. Written input mailed to the Working Group was coded and analyzed using the same protocols as the electronic data submitted over the Internet.
Analysis of the Data
Methods
The Working Group reviewed summaries of all the sources described above. The Community Meetings were considered, for analytical purposes, as case studies. In addition to the data on demographics and the votes recorded at each meeting, staff reviewed background information on each location and, in the course of planning each meeting, obtained a great deal of information on the health care, resources, and policy issues in each community. Senior staff members who attended the meetings used a structured format when preparing the meeting reports. The individual reports, including the data recorded at each meeting, are being made available to the public on www.citizenshealthcare.gov. The Working Group compared data across meetings only when it was truly comparable, that is, questions were asked in the same context during the meetings, in the same form. (See Appendix B for more information.)
Staff coded and analyzed data from open-ended, on-line polls, and Interim Recommendation responses using standard statistical software. The Working Group reviewed summary data, as well as the results of analyses that reflected possible differences in response patterns related to demographic differences. The Working Group also reviewed data from relevant national polls and surveys.
Public Comments
The Interim Recommendations posted on the web site received over 8,000 responses, mostly via the Internet, but also by mail, from June 1 through August 31. These public comments were classified into response categories and analyzed; comments were also posted on the web site. Official feedback from advocacy organizations and professional associations were reviewed by the Working Group members as well as staff, and posted on the Working Group web site. A summary of the comments and the Working Group’s response to the comments is presented in Appendix G.
Limitations
People attending the Working Group Community Meetings or providing input in writing are more likely than others to be especially interested in health care, either because they, or their family members, have had concerns about their health care or insurance coverage, or because they work in the health care field. The people we heard from were, on average, more likely to be female and in or on the edges of the Baby Boom generation (age 45-64), and the proportion having bachelor degrees or advanced graduate degrees was much higher than in the population as a whole. And, while participation in Community Meetings by minority group members was fairly close to national percentages, representation of people who identified themselves as Latino or as African American among those submitting comments or poll data was lower. The proportion of people who were not covered by any form of health insurance, and the proportion receiving benefits through Medicaid, was also lower than the nation as a whole. Some of these limitations were addressed by holding meetings specifically designed to reach underrepresented populations (see above). And, as noted above, analysis of the data was performed to assess the extent to which demographic factors may have accounted for some of the findings.
A more serious issue is the inability to ensure that people providing input represent the full spectrum of views of all Americans, given that people who are sufficiently interested or motivated to provide input on health care and policy issues may not be typical of the population as a whole. The consistency of findings across many communities and between the poll data obtained through both the Working Group Internet site and the community meetings provides support for the view that we have heard from a significant segment of the American people. The consistency between findings from recent national polls and surveys provides even stronger support for the findings. However, the meetings, as well as the www.citizenshealthcare.gov data were designed to offer information to help frame discussion and responses to questions, whereas national polls and surveys generally do not serve this purpose. Therefore, the responses we have analyzed are not exactly comparable to other national poll data, even when the same, or very similar, questions are asked. Consequently, we do not claim that we know, with great certainty, the values and preferences of all Americans. Rather, we are basing our recommendations on a careful assessment of input from as many sources as feasible, from tens of thousands of people from all across the United States, taking into account the gaps or biases that may be reflected in the data to the best of our ability.
Working Group Community Meetings (table)
| Kansas City, MO |
January 17, 2006 |
| Orlando, FL | January 24, 2006 |
| Baton Rouge, LA | January 26, 2006 |
| Memphis, TN | February 11, 2006 |
| Charlotte, NC | February 18, 2006 |
| Jackson, MS | February 22, 2006 |
| Seattle, WA | February 25, 2006 |
| Denver, CO | February 27, 2006 |
| Los Angeles, CA | March 4, 2006 |
| Providence, RI | March 6, 2006 |
| Miami, FL | March 9, 2006 |
| Indianapolis, IN | March 11, 2006 |
| Detroit, MI | March 18, 2006 |
| Albuquerque, NM | March 20, 2006 |
| Phoenix, AZ | March 25, 2006 |
| Hartford, CT | April 6, 2006 |
| Des Moines, IA | April 8, 2006 |
| Philadelphia, PA | April 10, 2006 |
| Las Vegas, NV | April 11, 2006 |
| Eugene, OR | April 18, 2006 |
| Sacramento, CA | April 19, 2006 |
| San Antonio, TX | April 19, 2006 |
| Billings, MT | April 21, 2006 |
| Fargo, ND | April 22, 2006 |
| New York, NY | April 22, 2006 |
| Lexington, KY | April 25, 2006 |
| Cincinnati, OH | April 29, 2006 |
| Little Rock, AR | April 29, 2006 |
| Tucson, AZ | May 4, 2006 |
| Sioux Falls, SD | May 6, 2006 |
| Salt Lake City, UT | May 6, 2006 |
University Town Hall Meeting, March 22, 2006 (table)
| Participating Institutions* | |
| Boston University | Boston, MA |
| Drexel University | Philadelphia, PA |
| Emory University | Atlanta, GA |
| George Washington University | Washington, DC |
| Indiana University | Indianapolis, IN |
| Johns Hopkins University | Baltimore, MD |
| Louisiana State University | Baton Rouge, LA |
| Michigan State University | East Lansing, MI |
| Northwestern University | Evanston, IL |
| Ohio State University | Columbus, OH |
| Penn State University | Harrisburg, PA |
| Purdue University | West Lafayette, IN |
| Tulane University | New Orleans, LA |
| University at Albany | Albany, NY |
| University of Arkansas | Fayetteville, AR |
| University of Illinois | Urbana, IL |
| University of Iowa | Iowa City, IA |
| University of Louisville | Louisville, KY |
| University of Michigan (Host) | Ann Arbor, MI |
| University of Minnesota | Minneapolis, MN |
| University of South Carolina | Columbia, SC |
| University of Wisconsin | Madison, WI |
* Not all meetings took place at main campuses.
Special Topic Community Meetings (table)
| Hanover, NH | Last Days | March 31, 2006 |
| Redwood Valley, CA | Native Americans | April 20, 2006 |
| Washington, DC | National Association of Realtors | May 16, 2006 |
| Atlanta, GA | Mental Health | May 22, 2006 |
Meetings Organized/Facilitated by Individual Members (table)
| Washington, DC | Ascension Health CEOs | December 5, 2005 |
| Daytona Beach, FL | Bethune-Cookman College | March 26, 2006 |
| Deltona, FL | Florida CHAIN (Community Health Action Information Network) and MS-keteers Multiple Sclerosis Support Group | May 6, 2006 |
| Palm Beach Gardens, FL | Area Agency on Aging | May 10, 2006 |
| Boca Raton, FL | Area Agency on Aging | May 11, 2006 |
| Lake Worth, FL | Area Agency on Aging | May 12, 2006 |
| Thousand Oaks, CA | City of Thousand Oaks Conejo Recreation and Park District | May 18, 2006 |
| Miami, FL | The Alliance for Human Services, The Human Services Coalition, Florida CHAIN, Miami-Dade County Health Department, Health Foundation of South Florida | August 22, 2006 |
Self-Initiated Meetings (table)
| Crossville, TN | The Learning Community | January-March, 2006 |
| Galena, IL | League of Women Voters | February 23, 2006 |
| Starkville, MS | MSU Extension | March 21, 2006* |
| Verona, MS | MSU Extension | March 27, 2006* |
| Wesson, MS | MSU Extension | March 29, 2006* |
| Hattiesburg, MS | MSU Extension | March 30, 2006* |
| Clarksdale, MS | MSU Extension | April 11, 2006* |
| Palm Beach Gardens, FL | Human Resource Association of Palm Beach County | April 11, 2006 |
| Greenville, MS | MSU Extension | April 18, 2006* |
| Newton, MS | MSU Extension | April 20, 2006* |
| Cloverdale, CA | United Church of Cloverdale | April 23, 2006 |
| Eau Claire, WI | Chippewa Valley Technical College | April 29, 2006 |
| Seattle, WA | Association of Advanced Practice Psychiatric Nursing | April 29, 2006 |
| Alpena, MI | League of Women Voters | May 1, 2006 |
| Galveston, TX | Center to Eliminate Health Disparities, University of Texas Medical Branch | May 1-3, 2006 |
| Boulder, CO | Individuals | May 3, 2006 |
| McKeesport, PA | Mon Valley Unemployed Committee | May 11, 2006 |
| Muncie, IN | BMH Foundation and Partners for Community Impact | June 2, 2006 |
| Birmingham, AL | Greater Birmingham PDA/DFA, UFCW Local 1657 | June 22, 2006 |
| Corvallis, OR | Mid Valley Health Care Advocates |
July 20, 2006 |
| Birmingham, AL | Birmingham Friends Meeting | July 16, 2006 |
| Jackson, MS | MSU Extension | August 22, 2006* |
| Hattiesburg, MS | MSU Extension | August 23, 2006* |
| Greenville, MS | MSU Extension | August 24, 2006* |
| Cleveland, OH | North East Ohio Voices for Health Care | August 24, 2006 |
| Columbus, IN | Columbus Regional Hospital Foundation (2) | August 29, 2006 |
* Held under the auspices of the Mississippi State University Extension Service.
Community Meetings on Interim Recommendations (table)
| San Jose, CA eBay/PayPal |
July 20, 2006 |
| Oklahoma City, OK | August 1, 2006 |
| Milwaukee, WI | August 12, 2006 |
Locations of Community Meetings Across the United States (map)
The Dialogue
This chapter highlights public input on the four questions Congress specified that the Citizens’ Health Care Working Group ask the American people. The Working Group has reviewed all input it has received from community and other meetings, by Internet, by mail, in person, or by phone. Particular emphasis in this section has been given to information gathered in community meetings held throughout the nation, which Congress directed the Working Group to conduct before preparing its Interim Recommendations. Other survey data sources are discussed throughout this section, and they will also be highlighted in the Final Recommendations to Congress.
This chapter follows the organization of the "typical" meeting, which always began with a discussion of participants’ underlying values. The 31 community meetings varied slightly from site to site, reflecting differences in the participants’ interests and preferences. While the general structure of the meetings was similar, it evolved over time as the Working Group attempted to find more effective ways to gather the desired information. Meetings varied in length, with most meetings either three or four hours long, although some were shorter and a few longer. At all these meetings, discussions centered on the four legislatively mandated questions:
I. What health care benefits and services should be provided?
II. How does the American public want health care delivered?
III. How should health care coverage be financed?
IV. What trade-offs are the American public willing to make in either benefits or financing to ensure access to affordable, high-quality health care coverage and services?
Summary of Findings
The following common themes emerged from the community meetings and other sources of information collected from the American public by the Working Group:
Values
-
Underlying the discussion of the four legislative questions is the belief by virtually everyone in attendance at each community meeting that the health care system has at least some serious problems.
-
Over 90 percent of participants at community meetings and respondents to the Working Group’s poll believed that it should be public policy that all Americans have affordable coverage.
I. What health care benefits and services should be provided?
-
A clear majority of participants preferred that all Americans receive health care coverage for a defined level of services.
-
People at the community meetings frequently expressed strong support for increased focus on wellness and prevention services as part of "basic" coverage, rather than focusing only on treating sickness.
-
Participants at meetings continually emphasized the importance of a strong education component in health care and the management of health.
-
Individuals voiced support for a fairly comprehensive basic benefit design.
-
Although many participants recognized the need to do more to ensure that the health care provided is appropriate and delivered efficiently, they were also concerned about arbitrary limits on coverage and were not comfortable with bare-bones benefit packages.
-
Despite the reluctance of many to limit benefits, participants at meetings supported limiting coverage to services that have proven medical effectiveness.
-
Participants expressed some level of support for the idea that some people could pay for additional services outside the basic benefit package.
-
People wanted consumers to play an important role in deciding what should go into a basic benefit package.
-
Participants in some meeting sites discussed a potential role for a local board or other quasi-governmental entity in defining the basic level of services.
-
Participants expressed the desire to be involved in the management of their own health care and were willing to accept some responsibility for their medical decision-making.
II. How does the American public want health care delivered?
-
At the community meetings, individuals asked for a delivery system that is secure, transparent, easy to navigate, and treats the "whole person."
-
Affordability of care is a primary concern among participants.
-
Participants were troubled that many people did not have access to the health care they need.
-
Many participants cited complexity of the system as a contributing factor to the problems with the health care system.
-
Linked to confusion about the health care system was the lack of useful information to help individuals navigate the health care system.
-
Participants mentioned that they or others were not always treated with respect or dignity.
-
Participants frequently cited barriers to care related to their insurance coverage.
-
Participants told the Working Group that they want to feel secure knowing that when they or their families need care, they can get it without becoming impoverished.
-
Participants wanted all Americans to be able to get the right health care, at the right time, in a respectful manner.
-
Participants noted that being able to choose and maintain a stable, long-term relationship with a personal health care provider was critical.
III. How should health care coverage be financed?
-
Although the results differed across meeting sites, a majority of participants (ranging from 55 percent to 88 percent in the community meetings) believed that everyone should be required to enroll in either private or public "basic" health care coverage.
-
In almost every community meeting, a majority of participants supported the notion that some individuals should be responsible for paying more for health care than others. The most commonly mentioned criterion for paying more was income, but varying payment by income was supported by the majority of participants in fewer than half of the meetings where this question was discussed.
-
Views about employer-based coverage did not generally reflect a deep distrust of employers, but instead were intertwined with broader concepts of health reform.
-
At most meetings, participants stressed the importance of preventive care to reduce health care costs.
-
Participants at most meetings believed that individuals have a responsibility to manage their own care and use of services.
-
In many meetings, participants mentioned that individuals have a social responsibility to pay a fair share for health care.
-
Participants frequently stated that the problems of high costs rest with "price setters"—namely, prescription drug companies, insurers, and for-profit providers.
-
A commonly expressed view was that a simpler system would result in lower administrative costs.
-
Some support exists for investment by providers and the private sector in health information technology to increase system efficiency.
-
Participants expressed general support for individuals playing their part in controlling utilization and costs.
-
Individuals would like information about how to use health care better and more effectively.
-
At some meetings, participants supported providing incentives to patients to engage in healthy behaviors.
-
Participants expressed preferences for using medical evidence to decide which services are covered and provided.
-
There was general support for controlling prescription drug costs by limiting direct-to-consumer advertising of prescription drugs and using more generic drugs, when medically appropriate.
-
Support also existed for limiting expensive yet "futile" end-of-life care and instead providing palliative care.
-
In almost all community meetings, participants expressed the belief that changing the culture from sick care to well care—namely, by focusing on prevention, wellness, and education (in general, and health education in particular)—will reduce health care costs.
-
A commonly expressed view was that better use of advanced practice nurses and other non-physicians could save money and improve quality.
-
Participants believed that investing in public health would pay dividends in terms of reducing health care costs.
-
Support for limits on malpractice was expressed at some community meetings.
IV. What trade-offs are the American public willing to make in either benefits or financing to ensure access to affordable, high-quality health care coverage and services?
-
In most meetings as well as on the Working Group poll, a majority of participants expressed a willingness to pay more to ensure that everyone has access to affordable, high-quality health care. Overall, about one in three (28.6 percent of poll participants) said they were willing to pay $300 or more per year.
-
When asked to rank or choose among competing priorities for public spending on health, individuals—with few exceptions—were most likely to rank "Guaranteeing that all Americans have health coverage/insurance" as the highest priority.
-
When asked to evaluate different proposals for ensuring access to affordable, high-quality health care coverage and services for all Americans, individuals at all but four meetings ranked "Create a national health insurance program, financed by taxpayers, in which all Americans would get their insurance" the highest. Three other options generally ranked in the top four choices at the community meeting locations: "Expand neighborhood health clinics"; "Open up enrollment in national federal programs like Medicare or the federal employees’ health benefits program"; and "Require that all Americans enroll in basic health care coverage, either private or public."
Detailed Description of Findings
Values
Before focusing on the four legislative questions, all meetings began with a discussion of individuals’ underlying values and perceptions that generally centered on three questions:
- When asked how they would describe the U.S. health care system
today, 97 percent of attendees across all community meetings selected
"It is in a state of crisis" (64 percent) or "It
has major problems" (33 percent). In each of the 31 community
meetings, at least 88 percent selected one of these options. Overall,
only two percent said "It has minor problems,"
and one percent either said "It does not have any problems"
or had no opinion. Underlying the discussion of the four legislative
questions is the belief by virtually everyone in attendance at each
community meeting that the health care system has at least some serious
problems. This same concern has also surfaced in national
polls. A January 2006 New York Times/CBS poll found that 90 percent
of respondents said that our health care system needs fundamental
changes or to be completely rebuilt (56 percent and 34 percent, respectively).1
This finding has been fairly consistent over the past 15 years. However,
the Employee Benefit Research Institute’s annual Health Confidencet
Survey has found from 1998 to 2004 the percent of respondents rating
our health care system as poor has doubled from 15 percent to 30 percent.
2
- When meeting participants at all meetings were asked, "Should
it be public policy that all Americans have affordable health care
coverage?", 94 percent overall said "yes." Similarly,
in the Working Group’s poll, 92 percent either strongly agreed
(79 percent) or agreed (13 percent) with this statement. Over
90 percent of participants at community meetings and respondents to
the Working Group’s poll believed that it should be public policy
that all Americans have affordable coverage. As stated by
participants in the Orlando community meeting, "Health care is
a right and not a privilege." Seattle, Denver, and Philadelphia
meeting participants, among other locations, desired "cradle
to grave" access to health care.
- At many of the community meetings, participants were asked what they believed was the most important reason to have health insurance. Although the results varied by meeting site, individuals were more likely to choose the response "To protect against high costs" than they were to choose the response, "To pay for everyday medical expenses."
Figure 1 illustrates how participants’ responses varied across community meeting sites and the Working Group poll.
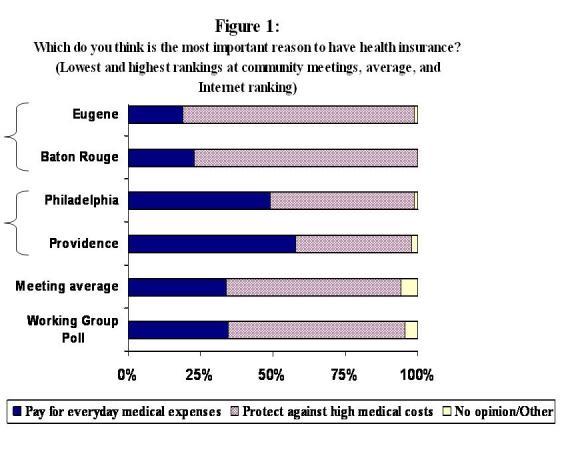
Note: This question was not asked in Los Angeles, Albuquerque, Hartford, Las Vegas, San Antonio, Fargo, Lexington, Little Rock, or Sioux Falls. Eugene and Baton Rouge were the meeting sites where "Pay for everyday medical expenses" ranked as the lowest among the cities where the question was asked, while Philadelphia and Providence were the meeting sites where that option ranked as the highest. The meeting average reflects a weighted average of all meetings where this question was asked.
What health care benefits and services should be provided?
Some common themes have emerged from the community meetings regarding what health care benefits and services should be provided. In the community meetings, discussion of this question generally revolved around three core questions.
The first of these questions is discussed below:
"Health care coverage can be organized in different ways. Two different models are: (1) Providing coverage for particular groups of people (e.g., employees, elderly, low-income) as is the case now; (2) Providing a defined level of services for everyone (either by expanding the current system or creating a new system). Which of the following most accurately reflects your views?"
In response to this question, a strong preference emerged:
-
A clear majority of participants preferred that all Americans receive health care coverage for a defined level of services. In response to the question, the vast majority (between 68 percent and 98 percent) of participants at all community meetings have said that we should provide a defined level of services for everyone. The highest level of support for a defined set of services was in the community meetings that were held in Philadelphia and New York, and the lowest in the Baton Rouge meeting (See Figure 2).
Figure 2:
Which statement best describes your views on how health care coverage should be organized?
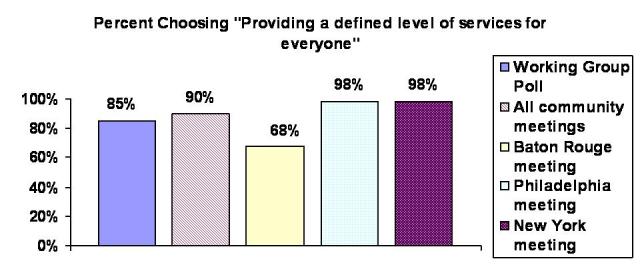
In the Working Group poll, 84 percent of participants answered the question this way. These findings are also consistent with the results of other national polls asking similar questions. In surveys conducted by other organizations, a clear majority have expressed the opinion that all Americans should have health insurance. For example, a Wall Street Journal poll regarding public support for a range of health practices in September 2005 found that 75 percent of U.S. adults somewhat favored (23 percent) or strongly favored (52 percent) universal health insurance.3 More recently, a New York Times/CBS poll conducted in January 2006 found that 62 percent said that they think the federal government should guarantee health insurance for Americans; 31 percent said this was not the responsibility of the federal government, and 7 percent said they do not know. 4
Discussions at community meetings teased out variations in how people conceptualize health coverage. For example, some participants indicated that it was hard to make a choice between the answers without knowing who was providing the coverage, or what would be covered. Many tended to view access to health care as a basic right, and they conveyed a willingness to contribute to the success of a system that would facilitate health care for all.
-
In the Baton Rouge community meeting, where the smallest percentage of people opted for providing a defined level of services for everyone, participants still concluded that a defined level of services for everyone was "more fair and equitable" in the face of the current system that was "failing."
-
In the Detroit community meeting, some participants worried that the issue of discrimination needed to be addressed, regardless of the system design. Just like the current system of providing coverage for particular groups of people (such as Medicare or Medicaid for elderly, disabled persons or low-income populations, or group coverage organized through employment), a system providing a basic level of care for everyone ran the risk of not providing sufficient levels of care for all. Participants expressed concern that any system reform must avoid creating different levels of care for different subsets of the population.
-
At the two largest community meetings in Los Angeles and Cincinnati, fewer than 10 percent of participants favored the current system that provides coverage according to a person’s affiliation with a particular group. These participants, like those at the other meetings, cited problems with the current system, including:
-
It excludes the unemployed and others who are not part of a particular group
-
The system is high cost, complex, and not uniform across groups
-
Mobility and flexibility are a problem.
-
-
About 90 percent of participants supported the option of providing a defined level of benefits for everyone, rather than the current system of coverage for certain groups. The virtues of implementing a system of coverage for all that were mentioned included:
-
Reduced overall and administrative costs
-
Decreased hospitalization and emergency room use
-
Access for all
-
Covered prevention and immunization, and
-
Improved level of national health care.
-
However, participants also expressed potential concerns about such a system, such as: What is the defined level of services? Who will be denied access to care if costs are too high, and who will make these decisions? Who will pay?
-
At all locations, participants emphasized the importance of involving consumers in the development of a basic benefit package. Because consumers can articulate what services are necessary at various stages of life, their participation in the development of the plan could help contain costs. In the Phoenix community meeting, for example, participants wanted a basic plan that would vary based on age and gender, and that could be added to if desired. Participants at most meetings recognized that the current system does work for some, and allows for a richer benefit than might be available otherwise, but that it does not work for everyone. They expressed a desire to build upon the current system, changing it into something that is more inclusive and provides a level of care for all Americans. Everyone would contribute to this system based on their ability to pay. However, for those people who are unable to afford the cost, government subsidies should be provided to allow access to a basic package.
-
In the San Antonio community meeting, participants expressed interest in an approach that would provide a basic level of care for everyone combined with personal responsibility.
-
In a number of community meetings, including Lexington, Eugene, Sioux Falls, and Cincinnati, participants commented that the United States should learn from other countries that have covered all or most of their citizens.
The second structured question delved into how to define the specific level of benefits:
"It would be difficult to define a level of services for everyone. A health plan that many people view as ‘typical’ now covers these types of benefits, many of which are subject to co-payments and deductibles: preventive care, physicians’ care, chiropractic care, maternity care, prescription drugs, hospital/facility care, physical, occupational, and speech therapy, and mental health and substance abuse. How would a basic package compare to this ‘typical’ plan? Are there benefits that you would add or would take out?"
Although the discussion differed by meeting location, some common themes emerged:
- People at the community meetings frequently expressed strong
support for increased focus on wellness and prevention services as
part of "basic" coverage, rather than focusing only on treating
sickness. According to participants at meetings throughout
the country, individuals have a responsibility to be good stewards
of their health and health care resources (preventive care/screenings/use
of services). They also viewed an emphasis on wellness and prevention
services as a way to reduce health care costs, as discussed in the
Financing section. According to these participants, disease management
should also be a part of the focus. In the Working Group poll, over
90 percent of respondents indicated that annual physicals and preventive
care should be part of a "basic" or "essential"
benefits package, a level of support that was similar to that for
hospital stays, prescription drugs, and lab tests.
- Participants at meetings continually emphasized the importance
of a strong education component in health care and the management
of health. To be good stewards of their health, individuals
need to be educated about wellness and prevention. People thought
information about how to use health care better and more effectively
was important, but not information on cost. Broader issues of general
education also came up in some meetings. Participants talked about
the importance of beginning early, in grade school, to focus on basic
skills that are prerequisites to literacy and health literacy. Fargo
meeting participants expressed a preference for "school-based
health promotion programs" for those in kindergarten through
grade 12.
- Individuals voiced support for a fairly comprehensive basic
benefit design. Benefits that a number of participants in
meetings throughout the country viewed as important components of
a basic benefit package included—but were not limited to—dental
care, vision, hearing, care by non-physician providers such as nurse
practitioners, long-term care, mental health, and hospice care. Some
meeting participants also desired coverage of complementary and alternative
medicine (for example, acupuncture).
- Although many participants recognized the need to do more to ensure that the health care provided is appropriate and delivered efficiently, they were also concerned about arbitrary limits on coverage and were not comfortable with bare-bones benefit packages. A participant in the Eugene community meeting made the point, "There’s a need for definition because we can’t afford it all." Still, when pressed to make decisions about what services to drop from basic coverage, many respondents told the Working Group "None," which was the most popular response in some locations.
| "All people should have the same coverage
that the President, Vice President, and Congress have…" (Phoenix meeting) "We agree that there should be a basic level of services for everyone- everyone has a right to that care. But our concern is that neither of those--what we have now, or a basic plan for everyone-- will work until it’s a consumer-driven choice and not a corporate solution that values profits above everything else. The consumer should be driving the choices, not like the way the culture is now. There should be more of a balance." (Charlotte meeting) "Every citizen has a basic right to have basic health care, and it can’t be based on the type of job they have." (Salt Lake City meeting) |
- Despite the reluctance of many to limit benefits, participants at meetings supported limiting coverage to services to those that have proven medical effectiveness. They expressed a certain level of comfort with decisions that could affect utilization, if they were based on medical evidence. Just over half of the Working Group poll respondents agreed (36 percent) or strongly agreed (14 percent) that health plans or insurers should not pay for high-cost medical technologies or treatments that have not been proven to be safe and medically effective, and nearly a quarter were neutral on the subject; responses in the March University town hall meeting were similar (see text box below), with 58 percent agreeing (36 percent) or strongly agreeing (22 percent).
University Virtual Town Hall Meeting:
"A National Conversation on Health Care"
| On March 22, 2006, 22 universities participated
in a simultaneous discussion on health care. Sponsored by the Big
Ten Conference and the Association of Schools of Public Health,
and hosted by the University of Michigan, this virtual town hall
meeting provided a forum for individuals across the country to voice
their opinions on health care. Broadcast via satellite from the University of Michigan, individuals participated in this event either by gathering at various university sites, or by logging onto the forum through the Internet. Interactive technology allowed various locations to call in with questions and comments, and individuals submitted their feedback through e-mail to be read during the live event. The 21 simultaneous meetings held in addition to the host meeting were organized by their respective university communities, and followed the same format. Participants at these meetings received the standard Community Meeting Discussion Guide and a Health Care Poll, specific to this event, which included the majority of questions asked on the Working Group’s own Internet poll (as well as in many of the Working Group Community Meetings). The separate meetings also had access to a local faculty expert who assisted in sending comments and questions to the national coordinator at the University of Michigan. After the event, the completed Health Care Polls were coded (772 from 22 of the webcast sites) and entered into a data set that was made available to the Working Group for analysis (See Appendix D for a complete summary of the results). Participating schools were: Boston University Drexel University Emory University George Washington University Indiana University Johns Hopkins University Louisiana State University Michigan State University Northwestern University Ohio State University Penn State University Purdue University Tulane University University at Albany University of Arkansas University of Illinois University of Iowa University of Louisville University of Michigan University of Minnesota University of South Carolina University of Wisconsin |
- Participants expressed some level of support for the idea that some people could pay for additional services outside the basic benefit package. For example, in Kansas City, participants favored allowing individuals to purchase additional coverage of chiropractic care or fertility treatments. Charlotte participants were willing to pay more for an "a la carte" plan that would allow people to add services to the basic plan, which could vary by life phases and would be most cost effective for each age group. At virtually every meeting, attendees expressed concern about coverage for "futile" care at the end of life.
Results of the Working Group poll question about the importance of including each of 23 specific benefits can be found in Appendix C (Question 4 of the Working Group poll).
The next question in this section of the community meetings asked participants for their views on who should decide which benefits would go into the basic benefit package:
"How much input should each of the following groups have in deciding what is in a basic benefit package (federal government, state and/or local government, medical professionals, insurance companies, employers, consumers)?"
Some common themes emerged in response to this question:
- People wanted consumers to play an important role in deciding what should go into a basic benefit package. In meetings throughout the country, the majority of participants consistently answered that a combination of consumers, medical professionals, federal government, state and local governments—generally in that order—should be responsible for having input into these decisions. Some participants indicated that employers and insurance companies should also play a role, but one that is more limited.
In the majority of meetings, participants were asked, "On a scale of 1 (no input) to 10 (exclusive input), how much input should each of the following have in deciding what is in a basic benefit package?" When participants were asked the question in this way, the highest rating was always for input from consumers, and it was always followed by "medical professionals."
| "Some new entity or process needs to
be created that includes all the relevant stakeholders, the foremost
of which would be the consumer." "[There should be] a ‘quasi-governmental’ entity representing all groups, including us, the people." "One way to organize this would be to create an entity very much like the Federal Reserve Board with appointed individuals who are professionals in their field and whose activities are generally public so it has to come under the federal government but wouldn’t be the government as we generally think of it." (Orlando meeting) |
Responses to this question are illustrated in Figure 3. In some meetings and on the Working Group poll, individuals were asked which party or parties they would prefer to make the decision regarding what services are covered in the basic health insurance plan. At least 60 percent of Working Group poll respondents and participants in the half dozen community meetings in which the question was asked this way chose the "some combination" option (of consumers, employers, government, insurance companies, and medical providers; the question did not identify which specific combination people preferred).
In the Sioux Falls meeting, participants were also asked to rate the "degree of involvement" government, medical professionals, insurance companies, employers, and citizens should each have in determining what is included in a basic health care package using the scale: major role, minor role, and no role. Consistent with other findings, 88 percent of participants voted that citizens should have a "major role," and 73 percent indicated that medical professionals should have a "major role." Participants generally believed that government (72 percent) and employers (64 percent) should play a "minor role;" insurance companies received a mixed response, with 55 percent saying they should play a "minor role" and 42 percent saying they should play "no role."
Figure 3 (table):
On a scale of 1 (no input) to 10 (exclusive input), how much
input should each of the following have in deciding what is in a basic
benefit package?
| Location | Federal Government |
State/Local Government |
Medical Professionals |
Insurance Companies |
Employers |
Consumers |
| Jackson | 3.6 |
3.0 |
5.7 |
1.8 |
3.6 |
7.8 |
| Seattle | 4.3 |
4.0 |
5.9 |
1.6 |
2.3 |
7.3 |
| Denver | 4.2 |
4.0 |
6.4 |
2.5 |
3.8 |
6.8 |
| Providence | 4.1 |
3.8 |
6.8 |
2.3 |
2.8 |
8.0 |
| Miami | 5.0 |
4.5 |
5.5 |
2.3 |
3.0 |
6.9 |
| Indianapolis | 4.9 |
3.9 |
6.1 |
2.2 |
3.3 |
7.6 |
| Detroit | 3.5 |
3.7 |
6.8 |
1.4 |
2.4 |
7.6 |
| Phoenix | 3.9 |
3.7 |
5.2 |
2.0 |
3.4 |
7.7 |
| Des Moines | 5.0 |
4.7 |
5.4 |
2.2 |
2.6 |
6.7 |
| Philadelphia | 4.4 |
4.4 |
6.0 |
1.5 |
3.1 |
6.7 |
| Sacramento | 3.8 |
3.8 |
6.4 |
2.5 |
2.9 |
7.4 |
| Billings | 5.1 |
4.7 |
6.0 |
2.4 |
4.0 |
6.3 |
| New York | 5.2 |
4.1 |
6.7 |
1.4 |
2.1 |
7.7 |
| Tucson | 3.9 |
3.4 |
6.2 |
2.6 |
3.2 |
6.6 |
| Salt Lake City | 4.6 |
4.7 |
4.9 |
2.6 |
3.1 |
6.8 |
| Average | 4.4 |
4.0 |
6.0 |
2.1 |
3.0 |
7.2 |
- Participants in some meeting sites discussed a potential
role for a local board or other quasi-governmental entity in defining
the basic level of services. For example, participants in
the Memphis community meeting strongly supported the concept of defining
the basic level of service using a "grass roots" method
through regional or state boards. In these discussions, participants
emphasized the need for a publicly accountable body.
- Participants expressed the desire to be involved in the management of their own health care and were willing to accept some responsibility for their medical decision-making. Meeting participants felt that consumers played an important role in decision-making. This opinion was expressed both by individuals who sought a larger role for government and those who preferred that government have a limited role.
Mental Health Meeting
| At its Boston meeting in August 2005, the Citizens’
Health Care Working Group heard from a panel made up of the Director
of Mental Health Services for Massachusetts, a representative from
a managed behavioral health care plan and an advocate for the mentally
ill. As members of the Working Group attended community meetings,
they heard that access to mental health services was a significant
issue to many participants. In order to delve more deeply into issues
related to mental health, the Working Group sponsored a meeting
focused on this topic in Atlanta, Georgia on May 22, 2006, at Skyland
Trail, a mental health facility which offers long- and short-term
residential care and community-based therapy, with the National
Mental Health Association of Georgia as a host. The participants at this meeting were knowledgeable about mental health. They included providers and consumers of mental health services, family members and advocates for the mentally ill and other health care providers. The meeting format was a mix of questions used at other community meetings and questions specific to mental health. Attendees believed that the value most fundamental to a health care system "that works for all Americans" is universal access, with health care as a right. Other important values are affordability and equal quality of care for all. In considering what was most important to the delivery of mental health care services, universal access was also the most important value, accompanied by integration of mental health into primary health care, parity for mental health care and eliminating the stigma attached to mental health. The issue participants believed most important to address in getting mental health care services is the lack of parity in insurance treatment of mental illness. Other problems that are priorities for action include the need for more funding for mental health services, the stigma associated with mental health conditions, continuity of care and the need for education to help people "know what is wrong and where to go for help." The inappropriate criminalization of mental health behaviors was also identified as a problem. When asked about the delivery of mental health services within the overall health care system, a majority of attendees embraced this vision which was developed by one table of participants: |
A comprehensive delivery system through primary care to include addictive disease, mental illness and all other physical illnesses with: |
|
| Ultimately, attendees wanted a system of "any door" access to services where dollars follow the consumer, and there is a focus on wellness recovery and resiliency. |
How does the American public want health care delivered?
In general, community meeting discussions of how the public wants health care delivered have been structured around two central questions. The first is discussed below:
"What kinds of difficulties have you had in getting access to health care services?"
Individuals at the community meetings discussed a number of problems
they or their family members have had in getting access to health
care services. Some common themes emerged that are summarized below.
| "When you change insurance, you should
be able to keep your doctor." "Primary care doctor—I like that relationship and I don’t want to see that go away." (Charlotte meeting) "It is an accident of history that medical insurance is attached to the place of employment, only to be lost or changed if jobs change or are lost." (Comments submitted to CHCWG Internet "What’s Important to You?") |
-
At the community meetings, individuals asked for a delivery system that is secure, transparent, easy to navigate, and treats the "whole person." Having a continuing relationship with a personal physician is just one component of a stable system, according to the participants. Confidentiality of medical records was mentioned as another important component of a good health care system. Individuals expressed a desire for a system that is holistic, treating the whole person rather than just treating "a bundle of symptoms," as described in the Denver community meeting.
-
Affordability of care is a primary concern among participants. At meetings throughout the country, individuals discussed how costs had prevented them or others from getting needed care. Costs of care generally referred to their (or their family’s) costs, including co-payments, deductibles, and health insurance premiums, rather than system-wide costs. Participants in different cities indicated that the high costs of prescription drugs were a particular concern. Participants in the Salt Lake City meeting discussed how "people are being priced out."
| "More than anything at our table
we have been talking about the cost of the health care –
cost is keeping people from getting the care." (Phoenix meeting) "We want health care delivered equitably at the community level by people we trust." (Memphis meeting) "We have rural areas here in Indiana where you can’t even get a paramedic." "We have lost time-intensive care. Providers right now don’t have time to spend with us! You only get two minutes with your doctor." (Indianapolis meeting) |
National polls have shown that the cost of health care overshadows concerns about quality. In fact, almost three-quarters (73 percent) of those surveyed in a 2005 Gallup Poll said they were greatly concerned about cost; less than half rated other items such as medical errors or avoidable complications, privacy of health information, or availability and access to services as great concerns.5 The EBRI 2004 Health Confidence Survey found that 34 percent of respondents were not at all confident (23 percent) or not too confident (11 percent) in their ability to afford health care today. The figure rose to 44 percent (25 percent not at all confident and 19 percent not too confident) when the respondents were asked about being able to afford care ten years out.6 For the last twenty years, a variety of survey findings consistently showed that approximately one in four Americans reported problems paying medical bills in the previous year.7 Surveys have continued to describe that burden Americans are feeling as it relates to the costs of medical care. According to a 2006 CBS/New York Times Poll, 61 percent of adults said they were concerned a lot about the health care costs they are facing now or will face in the future,8 A Pew Center for the People and the Press Survey found that 54 percent of U.S. adults reported that the costs of paying for a major illness was a major problem and 38 percent said even routine care was a major problem. Moreover, 70 percent of respondents said that the government spends too little on health care, while 65 percent thought that the average American spends too much. 9
| "Culturally competent care-funding
to encourage more minority physicians and providers. If I want
an African American dermatologist, I have to search high and low." (Indianapolis meeting) "You can’t get through this system without luck, a relationship, money, and perseverance." (Salt Lake City Meeting) "Care should be delivered at the most local level possible." (New York Meeting) |
-
Participants were troubled that many people did not have access to the health care they need. Access to care includes access to both facilities and health care providers, including specialists. Participants in community meetings nationwide highlighted problems with access to health care in rural areas, including lack of transportation to providers or facilities located far away. The lack of public transportation was brought up as an issue not only for rural areas, but for urban areas as well. Others described problems finding an accessible provider who was willing to accept their insurance, particularly Medicaid. Providers and facilities tend to be concentrated in suburbs and more populated areas. For example, in the Phoenix community meeting, individuals noted that most providers and specialists were concentrated in the Phoenix area, and it was difficult to access care in other areas of the state. According to a national Wall Street Journal/Harris Interactive survey 56 percent of adults agree that people who are unemployed and poor should be able to get the same amount and quality of medical services as people who have good jobs and are paying substantial taxes. 10
Consolidated Tribal Health Project, Redwood Valley, California
| "I don’t have money to get
my kids milk and you want me to take them to the dentist?" "Society preaches prevention—but a doctor isn’t going to see this young lady’s kids for preventive care. She might get in at a walk-in clinic, but what’s the quality of care? Is the waiting room safe? Is the provider credentialed? Are they culturally sensitive to your needs? We get referred to the outside world where they assume you can read and write and just have you signing forms and don’t take the time to explain it to you." Native Americans (both tribal and non-tribal members) met in Redwood Valley on April 20, 2006, at the Consolidated Tribal Health Project to provide an open, honest, and often emotional insight into the barriers they face in accessing even basic primary medical, mental and dental health care. Participants expressed their desire for everyone to have access to health care, both in terms of geographic distance and ability to access providers. They felt that "health care is not a privilege, it’s a right and we don’t receive that right…not only as Native Americans, but as rural citizens." Individuals addressed the issue of access as a multi-pronged problem. One woman said, "When they can afford to purchase gasoline, their tires are in good shape, and they aren’t in too much pain, they can make the long drive for care." If the primary care reveals a need for specialty services, they face an even greater hurdle. Individuals talked about how they valued culturally competent care with providers who took the time to explain medical terminology and did not assume literacy. One person noted that "[health] professional people are so professional that they don’t know how to relate to us nobodies. They don’t know how to tell us the simple things." Participants at this meeting emphasized the importance of the government recognizing its duty to the Native American population and honoring the trust relationship that is established in law. |
Mississippi Listening Sessions
| Eleven listening sessions organized by faculty
of the Mississippi State University Extension Service were conducted
between March 21, 2006 and April 20, 2006. These sessions were
held across the rural areas of the state and included a diverse
mix of geographies and cultures. Altogether, 138 people participated
in the sessions. The majority of participants were college graduates,
many with post-graduate education, and most had some form of health
coverage. Many of the participants were health care providers
or administrators, or business people actively involved in their
communities, and most were knowledgeable about the problems facing
low-income and underserved rural Mississippi communities. A major
thought expressed across the rural sessions was that many problems
with the health care system in rural areas are distinct from those
found in more urbanized areas. Lack of physicians and other health
care professionals, distances to services, transportation issues,
high cost, and lack of insurance were strongly recurring themes
across the state. Across the sessions, values regarding affordability and quality of care ranked highest among participants. Accessibility ranked third in urgency, but the total number of specific issues related to this concept dominated the discussion. Choice of care rounded out the list of values articulated at the sessions. Those observing the sessions noted that there were marked differences in the views expressed in the meetings, reflecting at least in part, differences in culture, but also the recent major devastation caused by Hurricane Katrina. Participants from the state’s southern regions, hardest hit by the storm, talked about problems they still face getting health care. Doctors left and patient records were destroyed or disappeared. And when some doctors attempt to return, they are finding that their patient base is scattered and possibly gone for good. Concerns were also expressed in the other regions of the state focused on the influx of Katrina and Rita evacuees (many of these evacuees are either uninsured or are covered by Medicaid) and the accessibility barriers that these people faced. Other storm concerns involved the lack of generators for respirators and difficulty accessing medication. One person who became the guardian after the storm of a 3-year old child who is covered by Medicaid seemed overwhelmed: "I don’t know what to do or how to access the system." Another left the same session highly distressed contending that, in light of this system’s inability to quickly respond to Katrina, we had no business focusing on health care issues that will take years to address, and that we should instead focus our attention on the possibility of other natural disasters, a potential pandemic, or a bioterrorist attack. In other sessions, people talked about more pervasive problems, including delays in the ability to schedule an appointment, and physicians who are unwilling to accept Medicaid or Medicare patients. Problems related to communicating with the system led one participant to advocate the establishment of patient navigators. One session in Hattiesburg focused on small businesses’ and independent contractors’ inability to secure reasonable group rates; it was mentioned that 28 percent of National Association of Realtors members have no health care coverage. Most participants (78 percent) agreed with the statement, "It should be public policy that all Americans have affordable health care." Compared to other meetings, however, participants expressed a stronger interest in focusing on personal responsibility (including taking advantage of educational opportunities) to improve health care and control health care costs, investing in public health infrastructure, and expanding safety net programs in order to ensure access to care. There was also a greater emphasis on expanding existing public programs and bolstering the employer-based health care system to address gaps in coverage, rather than initiating new programs or making fundamental changes to the health care system. The most resounding dialogue the group facilitators recalled at all the sessions focused on the availability of health care services. |
-
Many participants cited complexity of the system as a contributing factor to the problems with the health care system. A number of issues related to complexity were discussed. Some participants noted that a lack of transparency in insurance coverage and reimbursement policies contributed to the problems. In the Memphis community meeting, the discussion of the complexity of the insurance system emphasized the problems created by multiple payers. Related to the concept of multiple payers, participants in the Denver community meeting discussed how the "labyrinthine scheme of Medicare and Medicaid" sets up a system especially hard to navigate by or on behalf of elderly patients. In the Providence, Philadelphia, and Sacramento community meetings, the new Medicare prescription drug benefit (Part D) was cited as an example of the complexity of the health care system.
| "It’s so complex. You wake up one day and your contract has been renegotiated, your numbers have changed, and your providers have changed. There are too many rules and too much bureaucracy." |
- Linked to confusion about the health care system was the
lack of useful information to help individuals navigate the health
care system. Individuals wanted to have access to understandable
medical information to help them make educated decisions about their
health care. Many participants discussed their desire to partner with
their health care provider in making health care decisions. Participants
noted that sometimes it was very hard to find any information, although
we also heard from some participants that information was available
if one knew where to look. People often were not sure where to go
to find what they needed. The desire for information is not unique
to Working Group community meeting participants. According to a 2005
Gallup Poll, a slim majority (51 percent) of individuals said they
do not have enough information about hospitals and other health care
facilities to make educated choices for health care services. 11
- Participants mentioned that they or others were not always treated with respect or dignity. Examples of problems people encountered included a lack of effective communication, discrimination by race or ethnicity, long wait times, and overcrowded emergency rooms. In a number of locations, meeting participants discussed how they had encountered or knew of barriers due to race or ethnicity, language, lack of cultural sensitivity, and lack of health insurance.
| "It’s often more stressful to
deal with the insurance company than it is to deal with the disease."
(Des Moines meeting) "There should be no waiting period before becoming eligible for coverage." (Lexington meeting) |
- Participants frequently cited barriers to care related to their insurance coverage. People in community meetings mentioned that they have experienced problems getting care due to health insurance rules. For example, some services were not covered due to pre-existing conditions. Participants also discussed problems related to needing to go through an insurer’s gatekeeping requirements to receive referrals that sometimes were denied. A number of participants spoke of problems with the portability of health insurance under the current system. Within the employer-based health insurance system, someone who changes jobs might be forced to switch insurance and could lose access to their health care provider if that provider is not in the new network. Participants in the Billings community meeting noted that limited provider networks created access problems in Montana, a large but lightly populated state. In the Baton Rouge community meeting, participants noted that the experience from the hurricanes in the summer of 2005 brought to the forefront the need for major emergency preparedness in all aspects of the health care system, including among insurance providers.
The second question asked of community meeting participants about health care delivery relates to their priorities for getting needed care:
"In getting health care (choosing a physician, health
care provider, or health plan), what’s most important to you?"
The responses to this question built on the answers to the previous question about problems getting care. The primary themes related to affordability, accessibility, and forming mutually respectful relationships with providers.
- Participants told the Working Group that they want to feel secure knowing that when they or their families need care, they can get it without becoming impoverished. Discussants frequently mentioned that it was important that their out-of-pocket costs for health care not be unreasonably high. Participants said people should have to pay some amount, but they generally also said that patients of all income levels should be able to receive needed care without costs being a barrier.
| "I feel like we are only as good as
our weakest link, and so many people can’t afford care." (Fargo meeting) |
- Participants wanted all Americans to be able to get the
right health care, at the right time, in a respectful manner. Access
for everyone emerged as a common theme across meeting sites. Some
meeting participants said that receiving "the right health care"
meant that medical decisions would not be based on factors such as
a person’s age. Many participants decried making medical decisions
on the basis of cost rather than medical need, but did want the care
they receive to be delivered in a cost-effective manner. Participants
expressed the need to have care received in a coordinated and timely
manner. Among other factors, getting the right care in a respectful
manner involved having a provider who was courteous and could communicate
well. As stated in meetings from Charlotte to Seattle, participants
believed that care should be sensitive to the needs of different cultures.
The desire to be treated with respect has also been shown to be highly
valued in other national surveys. A 2004 Wall Street Journal/Harris
Interactive poll asked what qualities people believed were extremely
important from the doctors who treat them; some of the most popular
responses related to the medical provider’s interpersonal skills—such
as being respectful (85 percent) and listening carefully to health
care concerns and questions (84 percent). 12
- Participants noted that being able to choose and maintain a stable, long-term relationship with a personal health care provider was critical. Individuals at meetings throughout the nation reiterated the importance of the provider-patient relationship that they believed should not be affected by whether a person switches jobs or changes health insurance. In the Phoenix community meeting, participants valued being able to choose a provider that would listen to them and provide "true" care, rather than just writing out a prescription. They wanted to be able to keep their health care provider even if they changed insurance carrier. In a number of locations (such as at the meetings in Orlando and Detroit), participants also discussed the importance of choosing a specialist. Participants at the community meetings told the Working Group that they placed a high value on having a "medical home" in which they can spend individual time with a provider. On the other hand, some participants at other meetings, such as San Antonio, expressed a willingness to forego some choice of primary care physician in exchange for lower costs or higher quality care.
How should health care coverage be financed?
Community meetings tended to devote a substantial amount of time to questions related to financing health care and controlling health care costs. The first of five questions that were commonly used in community meetings asks participants their opinion on whether everyone should be required to enroll in basic health care coverage:
"Should everyone be required to enroll in basic health care coverage, either private or public?"
Meeting participants had interesting discussions in response to this question:
-
Although the results differed across meeting sites, a majority of participants (ranging from 55 percent to 88 percent in the community meetings) believed that everyone should be required to enroll in either private or public "basic" health care coverage. Support for some form of mandated coverage is displayed in Figure 4. Fewer than half (47 percent) of the Working Group poll respondents agreed or strongly agreed with requiring everyone to enroll in health coverage, and another 21 percent said they were "neutral." Over 80 percent in the University town hall meeting said everyone should be required to enroll in basic (public or private) health care coverage.
Figure 4 (table):
Should everyone be required to enroll in basic health care coverage, either private or public?
Percent Saying "Yes": |
||
Less than 70% |
70-79% |
80% or More |
| Kansas City (60%) Baton Rouge (65%) Albuquerque (62%) Des Moines (55%) Las Vegas (56%) Eugene (65%) |
Orlando (74%) Jackson (74%) Seattle (77%) Denver (75%) Providence (76%) Miami (75%) Detroit (75%) Phoenix (79%) San Antonio (73%) Billings (74%) Fargo (74%) |
Memphis (83%) Charlotte (80%) Indianapolis (88%) Philadelphia (82%) Sacramento (81%) Lexington (80%) Cincinnati (86%) Little Rock (85%) Tucson (88%) Sioux Falls (82%) Salt Lake City (81%) |
Note: Los Angeles, New York, and Hartford are not included in this table. In the Los Angeles meeting, the responses were modified based on participants’ comments in the meeting. As a result, only 16 percent answered "yes" to the question, while 78 percent of the participants chose a third option that was offered by participants—that everyone automatically would have coverage under a national system, so, according to participants, the question was not applicable. For the same reason, the question was not completed in the New York meeting. In the Hartford meeting, the majority of participants abstained.
| "Enrolling everyone in a single pool
would spread costs and yield savings." (Providence meeting) "There should be progressive rates for health care, based on ability to pay, through income taxes, as part of a single- payer system." (Hartford meeting) "All individuals should carry their own health insurance as they do for car and property. Insurance companies should be forced to insure individuals rather than corporate entities and employer groups." (Comments submitted to CHCWG Internet "What’s Important to You?") |
Several common themes emerged when individuals discussed why they supported requiring everyone to have health care coverage. Some participants expressed the opinion that those who are able should pay their fair share. At meeting sites throughout the country, individuals made the analogy to the law that requires everyone who drives to have automobile insurance. They believed that health coverage should be treated similarly since everyone uses health services. Additional analogies included laws requiring seat belt use and vaccinations, as expressed by meeting participants in Miami. Participants in community meetings in places such as Jackson and Denver that supported an "individual mandate" (in other words, a law requiring all individuals to have health insurance coverage) said it would be consistent with the philosophy of individual responsibility.
Younger Americans Weigh in on the Issues
| Over 100 students in an undergraduate public
health class at Purdue University participated in the University
town hall meeting as part of a class assignment. They completed
the University town hall poll, and explained their responses to
questions about policy options in essay questions. Compared to older respondents, the students were less likely to describe the health care system as being in a state of crisis (6 percent) or having major problems (61 percent). Most (88 percent) agreed or strongly agreed that it should be public policy that all Americans have affordable health care insurance or other coverage, and most (72 percent) said coverage should be provided for everyone, for a defined level of benefits. The students also opted, by a majority of 70 percent, for mandatory enrollment in some form of public or private coverage. The majority (57 percent) thought some people should be responsible for paying more for coverage than others, with respondents most likely to state that the criteria for paying more should be either health behaviors or income. The most important priorities identified by the students for public spending on health and health care in America were guaranteeing that all Americans get health care when they need it through some sort of private or public program and investing in public health programs to prevent disease, promote healthy lifestyles, and protect the public during epidemics and disasters. |
Although strong support for an "individual mandate" was found at each of the meetings, some participants disagreed. Others objected to the way the question was worded since they said it assumed implicitly that a national health care system would not exist. In fact, at the community meeting in Los Angeles, the vast majority of participants supported a new "third" option: that everyone automatically would have health coverage and access to care under a new national system. Participants who disagreed with the individual mandate concept expressed concerns that it would give greater power to the government and would undermine concepts of individual freedom. Someone at the Billings meeting noted, "[Montanans] don’t like to be told what to do." Meeting participants also expressed uncertainty about how undocumented persons or non-citizens would be treated in the individual mandate system, with some saying these individuals should receive care, others maintaining that non-citizens should not be entitled to coverage.
The next commonly asked question related to whether people should pay more for health care and, if so, whether the amount they should be required to pay should be influenced by income or other factors:
"Should some people be responsible for paying more than others? What criteria should be used for making some people pay more?"
-
In almost every community meeting, a majority of participants supported the notion that some individuals should be responsible for paying more for health care than others. The most commonly mentioned criterion for paying more was income, but varying payment by income was supported by the majority of participants in fewer than half of the meetings where this question was discussed. (See Figure 5.)
However, in many community meetings, no consensus emerged regarding who should pay more, as shown in Figure 6.
-
The most popular choice of criteria was income. In other words, those with higher incomes should pay more than those with lower incomes. Some participants argued that those with very low incomes should not have to pay anything for their care. A July 2006 Wall Street Journal Online/Harris Interactive Poll found that 39 percent of adults agree that the higher someone’s income is, the more he or she should expect to pay in taxes to cover the cost of people who are less well off and are heavy users of medical services. 13
-
The next most popular criterion often was health behaviors. Such a system could be structured either by reducing health insurance costs for those who practice healthy lifestyles (for example, exercising regularly, not smoking, wearing seat belts, etc.), or by increasing health care co-payments or premiums for those who practice unhealthy behaviors, such as smoking. (In three of the community meetings, the choice "other" was changed to "other/combination of factors," which could include both income and health behaviors, as well as other factors.) According to a Wall Street Journal Online/Harris Interactive Poll conducted in July 2006, more than one in three agreed (35 percent) but another 35 percent disagreed that it is unfair to require the majority of people who are healthy to pay for most of the cost of treating those who are sick and heavy users of hospitals and doctors. 14
Figure 5 (table):
Should some people be responsible for paying more than others?
Percent Saying "Yes": |
||
Less than 60% |
60-69% |
70% or More |
| Indianapolis (58%) Sacramento (43%) |
Orlando (64%) Baton Rouge (60%) Memphis (66%) Jackson (60%) Denver (66%) Miami (63%) Phoenix (65%) Tucson (61%) |
Kansas City (72%) Charlotte (72%) Seattle (77%) Providence (79%) Detroit (81%) Des Moines (73%) Philadelphia (83%) Billings (76%) Salt Lake City (80%) |
Note: This question was asked only in the above cities. In most meetings where this question was asked, participants were also asked which criteria should be used. In some meetings, however, only the question about criteria was asked. See the next question below.
Over 80 percent of respondents in the University town hall meeting said that some people should be responsible for paying more for coverage than others, and about 71 percent said income should be used as a criterion for making people pay more.
Figure 6 (table):
What criteria should be used for requiring some people to pay more?
Location |
Noneeveryone should pay same |
Vary by Family size |
Vary by health behaviors |
Vary by income |
Other |
Other/ Combination |
| Orlando | 21% |
6% |
15% |
41% |
17% |
Not asked |
| Baton Rouge | 6% |
15% |
27% |
44% |
8% |
Not asked |
| Memphis | 15% |
3% |
11% |
58% |
14% |
Not asked |
| Charlotte | 12% |
1% |
27% |
32% |
27% |
Not asked |
| Jackson | 26% |
4% |
19% |
38% |
13% |
Not asked |
| Denver | 16% |
4% |
16% |
57% |
8% |
Not asked |
| Los Angeles | 20% |
4% |
11% |
51% |
15% |
Not asked |
| Providence | 20% |
2% |
27% |
45% |
6% |
Not asked |
| Indianapolis | 16% |
4% |
29% |
47% |
5% |
Not asked |
| Detroit | 12% |
7% |
7% |
69% |
7% |
Not asked |
| Phoenix | 26% |
2% |
12% |
52% |
8% |
Not asked |
| Des Moines | 17% |
4% |
16% |
61% |
3% |
Not asked |
| Philadelphia | 8% |
5% |
7% |
70% |
10% |
Not asked |
| Billings | 12% |
7% |
29% |
44% |
8% |
Not asked |
| Fargo | 6% |
1% |
11% |
21% |
-- |
61% |
| Little Rock | 11% |
5% |
6% |
15% |
-- |
62% |
| Tucson | 18% |
0% |
18% |
50% |
13% |
Not asked |
| Sioux Falls | 13% |
3% |
23% |
10% |
-- |
52% |
| Salt Lake City | 9% |
4% |
23% |
59% |
6% |
Not asked |
Note: Figures may not add up to 100 percent due to rounding. Question was not asked in Kansas City, Seattle, Miami, Albuquerque, Hartford, Las Vegas, Eugene, Sacramento, San Antonio, New York, Lexington, or Cincinnati.
On the Working Group poll, there were multiple questions about how higher income people might pay more for coverage. About 40 percent (38 percent) of respondents agreed or agreed strongly that everyone should pay the same for health insurance, while 44 percent disagreed or strongly disagreed. When asked whether people with higher incomes should pay higher premiums for employer-sponsored health insurance, 37 percent agreed or strongly agreed, while 43 percent of respondents disagreed or strongly disagreed. Moreover, about one-third (34 percent) of respondents agreed or strongly agreed that higher income people should pay higher premiums for health insurance they buy themselves, compared to 45 percent who disagreed or strongly disagreed.
The level of support for higher-income people paying more for health insurance they purchase themselves was similar across education levels of the people responding to the Working Group poll. A large share of respondents disagreed or strongly disagreed. These findings may reflect the view, also heard at many meetings and in comments submitted via the Working Group poll, that there is some support for higher contributions from higher-income people, but there is less support for direct income-related cost-sharing or premiums than there is for contributions to a national coverage system through some form of progressive tax, as discussed below.
According to a recent Los Angeles Times/Bloomberg survey 34 percent of adults believe that it is the government’s responsibility to ensure that all citizens have health insurance and income for retirement, while 28 percent believe that it is the employer’s responsibility and 28 percent believe that it is the individual’s responsibility.15
The following question generated substantial debate at many of the meetings:
"Should public policy continue to use tax rules to encourage employer-based health insurance?"
As shown in Figure 7, the percent of individuals who agreed with this question varied greatly from meeting site to meeting site. In the Detroit community meeting, only 23 percent of participants supported a continuation of the use of tax rules to encourage employer-based health insurance, while 87 percent of those at the Baton Rouge community meeting agreed with the policy. In a number of meetings, some participants abstained from answering the question, in many cases because of frustration with the way the question was worded, as was the case with the previous two questions. In five of the community meetings, an "abstain" option was provided to participants.
A different question, focusing on whether employers should be given additional incentives to expand coverage, was asked in both the Working Group’s poll and the University Internet town hall meeting. Support for tax incentives for employer-sponsored coverage as a means of expanding coverage was relatively high. Almost 70 percent (69 percent) of Working Group poll respondents and 61 percent of University town hall meeting respondents agreed or strongly agreed with the strategy.
Figure 7:
Should public policy continue to use tax rules to encourage employer-based health insurance?
Percent Saying "Yes": |
||
Less than 30% |
30-49% |
50% or More |
| Memphis (29%) Providence (27%) Detroit (23%) Hartford* (15%; 41% abstained) Des Moines (24%) Las Vegas (25%) San Antonio* (14%; 48% abstained) |
Kansas City (36%) Seattle (32%) Denver (39%) Los Angeles (37%) Indianapolis (31%) Albuquerque (39%) Philadelphia (32%) Eugene (32%) Billings (46%) Fargo* (44%; 27% abstained) Little Rock* (42%; 23% abstained) |
Orlando (60%) Baton Rouge (87%) Charlotte (62%) Jackson (72%) Miami (67%) Phoenix (53%) Lexington* (63%; 18% abstained) Cincinnati (50%) Tucson (50%) Salt Lake City (53%) |
Note: Question was not asked in Sacramento, New York, or Sioux Falls. * "Abstain" option provided.
| "I do believe all employers large and
small should give their workers insurance. There should be programs
or better tax cuts for those employers." "[Expand] tax incentives for companies that provide health care benefits for their employees. Small companies should be able to join together to take advantage of group rates. Corporations like Wal-Mart should be penalized for not providing decent health care benefits for its employees." "If employers are to continue to provide coverage, all employers must participate, nationwide." "I think that placing the burden of health care on employers makes American businesses less competitive in the global market. At the same time, I think that placing the burden of paying for health care on individuals will ultimately drive up the cost of care by forcing the poor and middle-income among us to rely on costly emergency services that hospitals cannot ethically deny based on inability to pay, rather than cheaper preventive care which they can." "We must sever the relationship between health insurance and employment. Employers should not bear the cost; it is impacting our competitiveness in the global market and it leaves huge gaps in which persons not employed in a company providing health insurance, are forced to bear huge costs of non-group insurance or, most likely, go without insurance at all. The rising percentage of uninsured is a tragedy in itself because these people frequently go without needed health care until they reach crisis. In addition, we all pay for the uninsured through higher and higher insurance premiums. Our system must be completely overhauled and redesigned to provide universal coverage with buy-in by all who have the means and a safety-net for those who can not." (Comments submitted to CHCWG "What’s Important to You?") |
- Views about employer-based coverage did not generally reflect
a deep distrust of employers, but instead were intertwined with broader
concepts of health reform. The extent to which participants
at a meeting may have been more heavily focused on fundamental reform,
like a single-payer system, affected the group discussions about employer-based
coverage. An analysis of Internet and mailed-in, open-ended responses
to the question about changing the way health care is financed, as
well as comments from participants at some community meetings, revealed
at least four—sometimes overlapping—categories of responses.
- "The current system should be maintained or bolstered,
either on an ongoing basis or as part of a more comprehensive system."
Some meeting participants supported a clear role for
employers and a continuation of the current tax rules for employers.
Some participants who supported retention of these tax rules argued
that they needed to be applied fairly, with small businesses needing
additional incentives. Meeting participants who supported comprehensive
reform through some type of national plan told the Working Group that,
in the absence of a national plan, employers would need to be responsible,
with tax breaks provided to assist small businesses. Without a national
plan, participants worried that people across the country would lose
coverage through employers dropping insurance. In the community meeting
in Los Angeles, participants who supported continuing the current
tax system did so because they believed it encourages employers to
provide coverage that they might otherwise not have an incentive to
provide. They also felt that the system leads to higher employer productivity
and helps promote shared responsibility.
- "Employer-based insurance is not sustainable and
is too expensive." Many participants felt the nation
should move away from current tax rules that favor employer-sponsored
coverage. Even with the current tax breaks, health care costs continue
to rise rapidly, and both businesses and employees are footing ever
larger and unsustainable expenditures. Some meeting participants believed
that the system of employer-based health insurance needs to be replaced
to make U.S. industries more competitive. At least one person noted
that the employer subsidies were invisible to the average citizen,
unlike Medicare or Medicaid, whose costs are frequently cited. Other
participants noted that they were afraid to leave their jobs because
of fear of losing health insurance or paying higher premiums. Those
who opposed the current tax breaks cited a lack of equity in the current
employer-based insurance system, a system that, as long as it exists,
means that health care, as stated by someone at the Indianapolis meeting,
will be, "an imperfect patchwork full of gaps."
- "The whole system should be changed fundamentally, but employers should contribute through some form of taxation or contributions to a pool." Other participants indicated an interest in a non-employer based system, but one in which the employers are still involved. For example, in the Des Moines community meeting, a participant referred to the employment-based system as "…outdated and the money saved from not having an employer-based system could go towards higher salaries and/or taxes to create a new system." Some participants at different meetings supported fundamental change to the system, but believed that a transition period should be implemented during which employers would still contribute to the system.
| "We need to have one single pool of
Americans who are insured. This would help spread their risk and
everyone could be covered. Employers could contribute to the costs,
but individuals should be able to contribute on their own." (Comments submitted to CHCWG Internet "What’s Important to You?") |
- "Employer-based insurance is unfair, inequitable, and inadequate." A number of participants discussed other aspects of the employer-based system that were not working. For example, participants brought up the fact that some employers are going around the current tax system by hiring only part time employees, to whom they are not required to offer full benefits. In the Los Angeles meeting, many participants supported a government-run universal health care system because they felt that the current employer-based system is unfair. They expressed concerns that it excludes self-employed, unemployed, and part-time workers, and favors large corporations. These participants supported replacing the employer tax incentive with another type of tax (such as an income or payroll tax). At several meetings and in Internet comments, some called for a national value added tax(1) or national sales tax. A large number of participants expressed the opinion that access to care should not be tied to insurance coverage.
| "Employer-sponsored insurance worked
when it was a perk, an extra offered by employers. But now coverage
is a necessity, not a privilege." (Billings meeting) |
At some meetings, participants were asked what the responsibilities of individuals and families should be in a health care system. Although some of these topics will be discussed under the next question typically asked in community meetings ("What can be done to slow the growth of health care costs?"), the following section provides a brief summary of three of the most common responses to the question:
"What should the responsibilities of individuals and families be in the health care system?"
Three of the most common answers heard by the Working Group in response to this question were the following:
- At most meetings, participants stressed the importance of
preventive care to reduce health care costs. Preventive care
includes getting important screenings, exercising regularly if possible,
and following a healthy diet. Some individuals said that practicing
preventive care would lower health care costs.
- Participants at most meetings believed that individuals
have a responsibility to manage their own care and use of services.
Participants told the Working Group that doing so involves educating
oneself, possibly through attending health education classes. It also
involves being proactive in seeking better care and becoming wise,
informed consumers of health care services and following treatment
regimens. However, a number of participants noted that some people
are better equipped to be informed consumers than others.
- In many meetings, participants mentioned that individuals have a social responsibility to pay a fair share for health care. Participants in the Memphis and Las Vegas meetings, among others, mentioned that, in a universal health system, this would include paying appropriate and possibly additional taxes.
The Working Group poll also shows some support for strategies that focus attention on the costs and appropriate use of health care. A majority of respondents either agreed (37 percent) or strongly agreed (19 percent) that we should all pay for part of our health care costs so that we will be more careful about how we use health care services.
Hearing from self-employed small business owners
| The National Association of Realtors hosted
a community meeting during their annual legislative conference on
May 16, 2006, in Washington, DC, to enable the Citizens’ Health
Care Working Group to hear from these self-employed small business
owners from around the country. Participants at this meeting sought
to identify solutions for the problems specific to self-employed
small business owners. They recognized that more than one in four
of the nation’s 1.2 million realtors have no health care coverage,
while many others are only a single health incident away from having
their livelihood destroyed by high health care costs. Recurring themes in this meeting included a desire to have protection from financial ruin, having access to affordable care, and increasing the information available for patients on cost and quality to enhance their decision-making capabilities. They emphasized the need for a level of security in the health care system, saying that "we need something that ensures that if we become very ill, it doesn’t take away our livelihood or what we’ve worked so hard to earn all our lives." While most participants agreed that everyone should have access to basic health care services, they were rather evenly divided on whether or not people should be required to have health care coverage. One participant said that "at first I was going to say no (to a requirement), but then I thought, if they aren’t required to sign up for it then the only time they will get in the system is when there is emergency care and that will cost us more." Desiring to keep health care "in the competitive arena," participants talked about the need to have greater transparency in costs, standardization of forms, and understandable information to enable them to be better patients. There was a clear sentiment at this meeting to limit government involvement, with participants asking "has it ever improved anything if the government gets involved and standardizes it?" |
The next "typical" meeting question asked participants about ideas for reducing the growth of health care costs in this country:
"What can be done to slow the growth of health care costs in America?"
Participants had a variety of ideas about how they would slow the growth of health care costs. Throughout the meetings, common themes emerged:
- Participants frequently stated that the problems of high
costs rest with "price setters"—namely, prescription
drug companies, insurers, and for-profit providers. In meetings
throughout the country, participants mentioned the desire to limit
profits in the health care sector. Some participants also noted that
allowing the government broader authority to negotiate prices with
pharmaceutical companies would reduce Medicare costs. The Working
Group poll showed strong support for government setting limits on
prices for health care products such as prescription drugs or medical
devices; just over 70 percent of respondents strongly agreed (39 percent)
or agreed (32 percent) with these government-set limits. The general
lack of trust of for-profit health care expressed in the community
meetings is consistent with other national survey findings. For example,
a December 2003 Wall Street Journal Online Health Care Poll found
that most of the public do not view health care as a business that
should be driven by the profit motive, and only 22 percent would prefer
that for-profit insurance provide most health insurance; the findings
indicated a preference for government (31 percent) or non-profit organizations
(25 percent).16
- A commonly expressed view was that a simpler system would result in lower administrative costs. Participants believed that a more straightforward health care system would reduce administrative costs by eliminating duplication of services. At a number of meetings throughout the country, many individuals advocated a single-payer system to eliminate the middleman, possibly one structured like Medicare or similar to the public school system. Under this type of system, everyone would pay taxes to support the system, even though, as with education, they might not use the services. Participants advocating the single payer concept said it would be the most efficient way to organize health care.
| "I paid over $12,000 in expenses (not
including legal fees) to collect $12,500 in medical expenses because
insurers were arguing about who was responsible. Everyone wants
to avoid paying. It would be vastly cheaper to adopt any of the
European systems." "I think we'll finally, inevitably, follow the lead of every other Westernized nation and institute some form of extensive public health care system – I think it's the most efficient system, and the one that gives the best care to the most people. The biggest problem I see with the system as it now stands is that we as a society spend a huge amount of money putting a profit in the pockets of the ‘middleman’ in the system—the insurance companies. That's why we spend 50% more of our GNP on health care than other nations do while getting worse care, and it's absurd." (Comments submitted to CHCWG Internet "What’s Important to You?") |
- Some support exists for investment by providers and the
private sector in health information technology to increase system
efficiency. At a number of meetings, participants supported
increasing the availability of electronic medical records. Greater
investment in health information technology and moving to an integrated
system of electronic medical records could improve administration
and treatment and reduce medical errors, according to views commonly
expressed at the meetings. More than 70 percent (71 percent) of respondents
to the Working Group poll supported more investment by doctors, hospitals,
and other providers in health information technologies as a means
to improve quality and increase administrative efficiency. (By comparison,
a 2005 Wall Street Journal Online/Harris Interactive poll found that
78 percent of the public supported doctors’ use of electronic
medical records.)17
A concern discussed at some meetings was privacy of the electronic medical records, which is highlighted in recent national surveys. For example, a 2005 Harris Interactive poll found that 70 percent of Americans are very or somewhat concerned that personal medical information might be leaked due to weak data security, and the public was evenly divided on whether the potential benefits of electronic medical records outweigh the potential risks to privacy.18
Public investment in health information technology was not identified as among the priorities for public spending on health and health care by most Internet poll respondents (see Appendix C).
- Participants expressed general support for individuals
playing their part in controlling utilization and costs.
Individuals have a responsibility to be informed health care consumers
and comply with recommended treatments. To this end, participants
suggested several related ideas:
- Individuals would like information about how to use
health care better and more effectively. For example,
those with chronic diseases could use more information to properly
manage their treatments.
- At some meetings, participants supported providing incentives
to patients to engage in healthy behaviors. Some participants
supported the idea of rewarding people who practice healthy behaviors
(for example, not smoking, or getting recommended health screenings).
On occasion, participants also discussed the notion of penalizing
people who engage in unhealthy lifestyles. The type of unhealthy
behavior in question affected participants’ opinions, consistent
with other national surveys. According to a 2005 Wall Street Journal
Online/Harris Interactive poll, the majority of Americans supported
the idea of smokers, those who do not wear seat belts, and those
who drink alcohol heavily paying more in health insurance costs;
however, the same poll found strong opposition for charging more
to those who are overweight or who do not exercise regularly.19
According to a 2006 Wall Street Journal Online/Harris Interactive
poll that compared results from the same poll in 2003 to the results
in from the 2006 poll, in 2006 53 percent of adults agreed that
it is fair to ask people with unhealthy lifestyles to pay higher
insurance premiums than people with healthy lifestyles; while
in 2003 only 37 percent of adults agreed.20
- Participants expressed preferences for using medical
evidence to decide which services are covered and provided.
Many participants discussed the importance of focusing on evidence-based
medicine.
- There was general support for controlling prescription
drug costs by limiting direct-to-consumer advertising of prescription
drugs and using more generic drugs, when medically appropriate.
Participants at many meetings expressed the desire to limit or
prohibit direct-to-consumer advertising of prescription drugs,
which could reduce the over-use of heavily-advertised drugs and
slow the growth of health care costs. Some people mentioned ideas
to make generic drugs available more quickly in the market; for
example, Orlando community meeting participants suggested reducing
the length of time of the exclusive patent rights of pharmaceutical
companies.
- Support also existed for limiting expensive yet "futile" end-of-life care and instead providing palliative care. Participants at meetings generally recognized the high costs associated with certain end-of-life services, some providing little value to the patient despite their high costs. At the same time, they stressed the importance of pain management, hospice care, and other support services to improve the quality of the last days of life. Better communication with patients near the end of life was considered to be an important step in controlling these costs. Participants in some meetings stressed the importance of living wills and medical directives that detailed people’s wishes for treatment if they were too ill to communicate. At many meetings, similar concerns were expressed about the effectiveness and costs of care for very fragile newborns.
- Individuals would like information about how to use
health care better and more effectively. For example,
those with chronic diseases could use more information to properly
manage their treatments.
| "We should have the decency to honor
end of life by not pumping millions into the last days but rather
encouraging high quality comfort care." (Sioux Falls meeting) |
- In almost all community meetings, participants expressed the belief that changing the culture from sick care to well care—namely, by focusing on prevention, wellness, and education (in general, and health education in particular)—will reduce health care costs. Participants broadly supported greater emphasis on prevention as part of a "culture of wellness" in the health care system. A number of participants in community meetings across the nation (including Des Moines, Fargo, Salt Lake City, Las Vegas, and others) emphasized the need for education of both children and adults to make this culture possible.
| "If we want to bring the cost of health
care down, then ultimately, we need to reduce the burden of disease.
We need to reduce the need to spend money rather than figuring out
how to redistribute the money. Otherwise the system will remain
broken regardless of how we want to pay for it." (Indianapolis meeting) |
- A commonly expressed view was that better use of advanced
practice nurses and other non-physicians could save money and improve
quality. In some meetings, participants supported the increased
use of care provided by health professionals other than physicians
including greater use of home-based care.
- Participants believed that investing in public health would
pay dividends in terms of reducing health care costs. Some
people discussed providing more funding for community health centers
and for public health more generally. They believed that doing so
could reduce racial differences or disparities in health care, and
could effectively reduce overall system costs.
- Support for limits on malpractice was expressed at some community meetings. Some participants discussed decreasing malpractice costs.
| End-of-life care has surfaced
at virtually every community meeting as an issue that encapsulates
many of the frustrations with health care in America. Sometimes
meeting attendees discussed the need for hospice care in the basic
benefit package. Sometimes participants talked about exchanging
expensive measures of questionable efficacy for the dying for general
improvements in access to care. Usually, the speaker raising the
issue has been a bit tentative. "I’m not sure how to
phrase this…" or "This sounds clumsy…"
Death is a difficult topic among family and friends; it’s
also difficult in a policy context. At its Boston hearing, the Working Group heard a panel of experts on end-of-life care. This discussion was compelling, and members asked that a community meeting be held on the topic (information on the presentation can be found in Appendix E). This special topic meeting was held March 31, 2006 in Hanover, New Hampshire. About 120 people attended. "Living Well through the End-of-Life" was the theme of the meeting. The last chapter of many people’s lives requires support and assistance, but often what is needed to live well is not medical in nature. Transportation, personal care, and help with meals and cooking are all needed. What people attending the meeting feared most about their final days (or those of someone close to them) were intractable pain, "prolongation of death," and losing personal control. They identified potential challenges related to "getting the system to work for you when you are dying" or "graceful surrender." What people wanted most from the medical system was to have their choices honored, good pain relief, and respect from health professionals so they could maintain their dignity. The majority believed that family and friends are the primary sources of such help, but that some paid assistance should also be available. People would like respite services for the principal care provider and a contact person for coordination of community help. "Care has to be taken out of the medical system and accommodate what happens in the community." Most people (69 percent) wanted to die at home. Close to 85 percent believed that other choices could be acceptable if certain elements of care were well managed. When asked what policy advice they’d give their Senators, participants had many specific suggestions, such as realigning financial incentives so that physicians could be encouraged to spend more time talking to patients and a request to revisit Medicare hospice payment practices. However, suggestions quickly began to mirror what has been heard in other meetings. "As a health care consumer, I want appropriate, timely, comprehensive care from conception to death and I would be willing to pay an additional modest percentage of income across my working life to achieve this." |
A value added tax is a tax, levied at each stage of production, on the added value in each stage as firms produce goods or services. It is similar in some respects to a sales tax. Many industrialized nation employ various types of value added taxes. (See Bickley, James M. CRS Report for Congress Value-Added Tax: A New U.S. Revenue Source? Washington D.C: Congressional Research Service, August 22, 2006. Accessed at http://opencrs.cdt.org/rpts/RL33619.pdf.)
What trade-offs are the American public willing to make in either benefits or financing to ensure access affordable, high-quality coverage and services?
The last of the four questions that the legislation directed the Working Group to ask the American people is about trade-offs they are willing to make so that everyone has access to affordable, high-quality care. In community meetings, the "typical" structure was to ask participants to discuss their willingness to pay to achieve this goal, evaluate the most important priorities for public spending on health care, consider specific trade-offs the public would be willing to make, and then to evaluate potential approaches for improving access to affordable, high quality health care for all Americans. In many meetings, time constraints or the desire by participants to reiterate their support for broad system reform precluded discussion of some of these questions.
Many comments submitted to the Working Group via the poll provide additional context for understanding what we heard about trade-offs. Although worded in a variety of ways, the single most common response to the question about trade-offs can be summarized as "no trade-offs." The discussions at the community meetings provided context for what people really were saying, which is far more complicated.
The discussion at meetings was divided into several parts. One set
of deliberations at the meetings focused specifically on paying for
expanded coverage.
| "That is too broad a question. There
is the wealthy American public who have lots of options right
now. There is the less wealthy American public who have enough
income to take some of the available options. There is the working
American public who can just barely afford any available options.
And there is the American public who can not afford any of today's
health care options. And each group will have very different ideas
about what they are willing to give up or ‘trade-off’
to get affordable, good quality health care. Even the concept
of ‘quality’ health care is a relative term -- any
reasonably trained and mostly competent doctor looks good when
your choice is that doctor or no treatment at all. What all Americans
should want is at least the quality and availability of care that
countries like Canada, France, England, etc. offer." (Comments submitted to CHCWG "What’s Important to You?") "Eliminate profits in the health care system to pay for universal coverage." (New York City meeting) "Eliminate medical middlemen (insurance companies) and direct-to-consumer advertising by pharmaceutical companies in exchange for universal health care." (Hartford meeting) |
"How much MORE would you be willing to pay (taxes, premiums, co-payments, or deductibles) in a year to support efforts that would result in every American having access to affordable, high quality health care coverage and services?"
-
In most meetings as well as on the Working Group poll, a majority of participants expressed a willingness to pay more to assure that everyone had access to affordable, high quality health care. Overall, about one in three (29 percent) said they were willing to pay $300 or more per year. Sizable shares of participants expressed a willingness to contribute some additional amount each year toward the stated goal. (See Figure 8.) Although the size of the groups varied, some participants at all meetings said they would be willing to pay an additional $1,000 or more in a year. The Working Group poll indicated that 12 percent would be willing to pay $1,000 or more per year (in taxes, premiums, or deductibles) to support efforts that would result in access to affordable, high-quality health care services and coverage for all, and 17 percent would be willing to pay an additional $300 to $999. Another 19 percent said they did not know, and 13 percent said they would not be willing to pay anything extra.
| "For those that already have health
care, I believe many are willing to pay a little more for that
benefit if they can be guaranteed that the extra would be put
towards providing health care for those less fortunate; most of
us have been in the position of having no health care at one time
or another in our lives. For those that don't currently have health
care, there can't be much they can trade". "I think that most people would be willing to accept a national value added or national sales tax to fund a nationalized medical system that treats all legal citizens fairly and equally, without financial or any other kind of discrimination." "Phase it in. Universalize a small sector of health care--for example, preventive care--before trying to redo the entire system. If the public learns to trust a small sector of tax-financed health care, it will be more open to greater change." "It should be underwritten by the government, with sliding scale of payments made by individuals through taxes - people who make the most should pay the most to insure that health care is available for all; employers should also contribute through the taxes they pay." Comments submitted to CHCWG "What’s Important to You?") |
In the Working Group poll, the amount they were willing to pay was fairly consistent across age; however, persons with the highest levels of education (those with graduate degrees) were more likely to be willing to pay $1,000 or more than those with less education, a finding that could indicate that those likely to have more money are willing to pay more. It may also reflect that those with higher levels of education typically have richer employer-sponsored insurance packages, face lower out-of-pocket payments, and therefore have not already reached their limit in terms of willingness to pay. At the meeting with realtors (see "Hearing from self-employed small business owners" text box presented earlier), where few have any employer-sponsored insurance and face high premiums in the individual market, a large percentage were not willing to pay anything more, even though they earn relatively high incomes. Even so, in the 28 meetings where the question was asked, at least 43 percent of participants indicated some willingness to pay more to achieve this goal.
Figure 8 (table):
Amount Willing To Pay in a Year So That Every American Has Access to Affordable, High-Quality Health Care
| Location | $0 | $1-$99 | $100-$299 | $300-$999 | $1,000+ | Dont Know |
| Kansas City | 7% | 12% | 19% | 24% | 25% | 14% |
| Orlando | 18% | 11% | 20% | 15% | 17% | 20% |
| Baton Rouge | 9% | 20% | 20% | 26% | 20% | 7% |
| Memphis | 31% | 2% | 4% | 13% | 31% | 19% |
| Charlotte | 45% | 8% | 11% | 10% | 16% | 11% |
| Jackson | 34% | 16% | 15% | 13% | 5% | 18% |
| Denver | 12% | 16% | 17% | 24% | 25% | 6% |
| Los Angeles | 38% | 14% | 9% | 10% | 11% | 19% |
| Providence | 24% | 8% | 21% | 16% | 24% | 8% |
| Indianapolis | 12% | 15% | 15% | 16% | 22% | 20% |
| Detroit | 10% | 13% | 15% | 21% | 33% | 8% |
| Albuquerque | 22% | 8% | 18% | 18% | 24% | 10% |
| Phoenix | 19% | 15% | 20% | 19% | 20% | 7% |
| Hartford | 20% | 10% | 13% | 27% | 22% | 8% |
| Des Moines | 14% | 12% | 15% | 31% | 20% | 9% |
| Philadelphia | 9% | 12% | 12% | 13% | 28% | 25% |
| Las Vegas | 15% | 18% | 21% | 20% | 16% | 11% |
| Eugene | 13% | 12% | 12% | 18% | 33% | 12% |
| San Antonio | 8% | 15% | 23% | 20% | 19% | 15% |
| Billings | 15% | 16% | 19% | 19% | 21% | 10% |
| Fargo | 11% | 16% | 30% | 16% | 13% | 14% |
| New York | 25% | 3% | 6% | 13% | 36% | 16% |
| Lexington | 11% | 15% | 18% | 29% | 20% | 6% |
| Cincinnati | 24% | 19% | 15% | 10% | 12% | 19% |
| Little Rock | 14% | 26% | 23% | 18% | 7% | 12% |
| Tucson | 23% | 19% | 0% | 29% | 13% | 16% |
| Sioux Falls | 6% | 16% | 16% | 25% | 28% | 9% |
| Salt Lake City | 23% | 14% | 20% | 25% | 11% | 6% |
| AVERAGE | 19% | 14% | 16% | 17% | 19% | 14% |
| Working Group Poll | 13% | 17% | 21% | 17% | 12% | 20% |
Notes: Figures may not add up to 100 percent due to rounding. The "don’t know" data for the Working Group poll includes the one percent that did not respond. Question was not asked in the Seattle, Miami, or Sacramento community meetings.
The next question asked the public about its views on what should be the most important priority for public spending for health care:
"Considering the rising cost of health care, which of the following should be the most important priority for public spending to reach the goal of health care that works for all Americans?"
At community meetings throughout the country, participants were asked to consider a list of possible priorities for public spending to reach the goal of health care that works for all Americans. In some of the meetings, participants were asked to give the most important priority of those listed, while in other meetings participants were asked to rate each priority on a scale from 1 (low) to 10 (high). The list presented at the meetings generally included the following items: guaranteeing that there are enough health care providers, especially in areas such as inner cities and rural areas; investing in public health programs to prevent disease, promote healthy lifestyles, and protect the public in the event of epidemics or disasters; guaranteeing that all Americans have health insurance; funding the development of computerized health information; funding programs that eliminate problems in access to or quality of care for minorities; funding biomedical and technological research; guaranteeing that all Americans get health care when they need it, through some form of public or private program, including "safety net" programs for those who cannot afford care otherwise; and preserving Medicare and Medicaid.
Although the phrasing of the question and the options given were not exactly the same across the community meeting sites and the Working Group poll, the top priorities were consistent:
-
When asked to rank or choose among competing priorities for public spending on health, meeting participants—with few exceptions—were most likely to rank "Guaranteeing that all Americans have health coverage/insurance" at the top of the list. In the Working Group poll, 64.6 percent chose this as among the top three priorities for public spending on health.
-
Other spending priorities in the list that tended to score high included:
-
Investing in public health programs to prevent disease, promote healthy lifestyles, and protect the public in the event of epidemics or disasters
-
Guaranteeing that all Americans get health care when they need it, through some form of public or private program, including "safety net" programs for those who cannot afford care otherwise
-
Guaranteeing that there are enough health care providers, especially in areas such as inner cities and rural areas , and
-
Funding programs that eliminate problems in access to or quality of care for minorities.
-
It is important to note that each of the eight options provided by the Working Group likely would receive support from the public if polled separately, even if it did not rank as the highest priority among the group. For example, "funding the development of computerized health information" and "funding biomedical and technological research" generally did not rank among the highest priorities, though discussions at Working Group meetings frequently emphasized their importance. Similarly, individuals selecting other options as most important (such as "guaranteeing that all Americans have health insurance") would likely be in favor of strengthening Medicare and Medicaid as part of the broader health care structure that would cover all Americans.
It is also important to note that support for any of the particular proposals could change dramatically when the list of potential priorities was modified, as occurred in two meetings. In the Hartford meeting, where participants were asked, "Which is your first priority?" discussants there added a ninth priority to the list: "Guaranteeing that all Americans have quality health care." When this option was included in the list of options, a full 80 percent of participants selected it rather than the options ranked highly elsewhere. For example, although the option, "Guaranteeing that all Americans have health coverage" ranked as the second highest priority in the list, it was selected by only 8 percent of participants. "Guaranteeing that all Americans get health care when they need it" also was selected by 8 percent of respondents, and no other option generated more than one vote. Similarly, in the Billings meeting, audience members requested a word change of one of the choices to include "Guaranteeing that all Americans have health care." In this meeting, participants were asked to rate each priority on a scale from 1 (low) to 10 (high). When this option was added, it ranked higher than any other option.
Paying More Taxes for Health Care for All:
Evidence from Other National Polls
-
A poll conducted in December 2004 by The Pew Research Center for the People and the Press found that 65 percent of Americans favor or strongly favor the U.S. government guaranteeing health insurance for all citizens, even if it meant raising taxes (Pew); an earlier poll conducted in August 2003 also by Pew from the same polling group also found that 67 percent favored guaranteeing health insurance to all citizens even if it meant raising taxes. 21
-
A 2003 CBS News/New York Times poll showed that 81 percent of respondents favored using potential tax cut money to ensure all Americans have access to health insurance, whereas 14 percent indicated a tax cut should be a higher priority. 22
-
A 2003 poll found that 79 percent of Americans believed it is more important to provide health care coverage for all Americans, than to hold down taxes. (ABC/Washington Post). 23
The next question often asked at community meetings was met with resistance at most meetings, sometimes by many of the participants:
"Some believe that fixing the health care system will require trade-offs from everyone—for example, hospitals, employers, insurers, consumers, government agencies. By ‘trade-off’ we mean reducing or eliminating something to get more of something else. On a scale from 1 (strongly oppose) to 10 (strongly support), please rate your support of each of the following trade-offs. What are some other examples of trade-offs that you would support?"
In many of the meetings, the Working Group provided a list of specific trade-offs for participants to evaluate:
- Accepting a significant wait time for non-critical care to obtain
a 10 percent reduction in health care costs
- Paying a higher deductible in your insurance for more choice of
physicians and hospitals (or paying a lower deductible with less choice)
- Paying more in taxes to have health care coverage for all. This
could mean limiting coverage to high deductible/ catastrophic care
or, if you were willing to pay more, a more comprehensive package
- Expanding federal programs to cover more people, but providing
fewer services to those currently covered in those programs
- Limiting coverage for certain end-of-life care of questionable
value in order to provide more at-home and comfort care for the dying
- Having government define benefits and set prices versus relying on free market competition by doctors, hospitals, other health care providers, and insurance companies.
| "I would be more willing to pay more in taxes to assure that everyone has access to good healthcare if I could be assured that the medical care system was based on fair practices and was not influencing politics. I would be thrilled to see Americans embrace a healthier lifestyle. That is a trade-off that doesn't cost much. People seem to believe that they can just take a pill or wait for some breakthrough to solve their health problems. Public schools need to bring back physical education and increase activity, cities need to become more pedestrian/bicycle-friendly. This country can help provide the opportunity to MAINTAIN good health instead of fixing the problems of poor health; - it would be a lot cheaper. I'd be willing to pay more in taxes for things like that." (Comments submitted to CHCWG "What’s Important to You?") |
In a number of meetings, participants voiced support for limiting coverage for end-of-life care of questionable value in order to provide more at-home and comfort care for the dying. This option received strong support in both the Working Group poll and the University town hall meeting—59 percent and 63 percent, respectively, agreed or strongly agreed with the proposal. The proposal generally receiving the lowest level of support was "expanding federal programs to cover more people, but provide fewer services to persons currently covered by those programs." In the Working Group poll, for example, only 17 percent of respondents agreed or strongly agreed with this proposal. In the University town hall meeting, 24 percent agreed or strongly agreed.
Individuals at many, if not all, community meetings argued that there were enough resources in the system already to achieve a goal of health care that works for all Americans, that resources just need to be redistributed. Most, however, did not think that the resources needed to be redistributed away from services provided to them; rather, they wanted to see reductions in waste, fraud, and (unnecessary) profit. In other cases, participants thought that the trade-offs should come from outside the health arena. For example, at the Los Angeles community meeting, participants developed and voted on their own list of specific trade-offs they would be willing to support. The only two choices that garnered majority support were: (1) No trade-offs—the American people already pay more than enough to fully fund a single-payer universal plan; and (2) Trade war for health care—cut from defense and homeland security budgets. In Las Vegas, the participants opted for "re-evaluating federal spending priorities."
Despite the resistance to this particular question, the meeting participants did discuss various trade-offs (without using that term) in previous sections of the meeting. For example, as noted above, many participants expressed a willingness to pay more so that everyone had care. Many participants also told the Working Group that individuals should play a larger role in their health and health care. More than one in three people filling out the Working Group’s Internet poll said they would be willing to pay a higher deductible in exchange for more choice of providers and services. This level of support for a trade-off of out-of-pocket costs for choice was actually slightly higher than the 2004 National Opinion Research Center at the University of Chicago (NORC) national survey finding that 27 percent of respondents would be willing to accept a higher deductible in exchange for fewer restrictions on use. The NORC results varied by income: 40 percent of Americans with household income of $75,000 or more would accept a higher deductible, compared with 23 percent with income below $25,000.24 The Working Group was not able to analyze the relationship of income to its participants’ responses.
The final substantive question at meetings asked people for their opinions on a range of fairly specific yet broad proposals for ensuring access to affordable, high quality health care coverage and services for all Americans:
"If you believe it is important to ensure access to affordable, high-quality health care coverage and services for all Americans, which of these proposals would you suggest for doing this?"
As with the previous question, participants at the community meetings were asked to evaluate a list of proposals. In this case, participants were asked to evaluate ten proposals on a scale from 1 (low) to 10 (high). Proposals included: offer uninsured Americans income tax deductions, credits, or other financial assistance to help them purchase private health insurance on their own; expand state government programs for low-income people, such as Medicaid and the State Children’s Health Insurance Program (SCHIP), to provide coverage for more people without health insurance; rely on free-market competition among doctors, hospitals, other health care providers, and insurance companies rather than having government define benefits and set prices; open up enrollment in national federal programs like Medicare or the federal employees’ health benefits program; expand current tax incentives available to employers and their employees to encourage employers to offer insurance to more workers and families; require businesses to offer health insurance to their employees; expand neighborhood health clinics; create a national health insurance program, financed by taxpayers, in which all Americans would get their insurance; require that all Americans enroll in basic health care coverage, either private or public; and increase flexibility afforded states in how they use federal funds for state programs—such as Medicaid and SCHIP—to maximize coverage.
As with the question on priorities for public spending, preferences varied somewhat in different meetings and on the Working Group poll. Once again, however, a clear consensus emerged among these options:
- When asked to evaluate different proposals for ensuring access to
affordable, high-quality health care coverage and services for all
Americans, individuals at all but four meetings ranked "Create
a national health insurance program, financed by taxpayers, in which
all Americans would get their insurance" the highest.
- Three other options almost consistently ranked in the top four choices:
- Expand neighborhood health clinics
- Open up enrollment in national federal programs like Medicare
or the federal employees’ health benefits program, and
- Require that all Americans enroll in basic health care coverage, either private or public.
- Expand neighborhood health clinics
These options received high levels of support, in the community meetings as well as the Working Group poll. The support for neighborhood health clinics and for opening up enrollment in Medicare or the federal employees’ health benefits program was consistently high and in line with the strong support for the Medicare program that was expressed in meetings across the country. The responses to both the Working Group poll and the University town hall meeting were similar to each other, as shown in Figure 9 below. There was, however, stronger support for expanding state programs such as Medicaid or SCHIP in the poll and the University town hall meeting than in the 31 community meetings. The level of support in the Working Group poll and University town hall meeting for opening enrollment in national programs such as Medicare or the federal employees’ health benefits program was in line with a 2005 national survey by the Employee Benefit Research Institute that found 76 percent strongly or somewhat favor allowing uninsured people to buy into government programs such as Medicare and Medicaid, or into the one in which members of Congress participate. 25
In the community meetings, the individual mandate (in other words, requiring that all Americans enroll in basic health care coverage, either private or public) was included as one of the options. Regardless of when in the meeting the question was asked, this option had a fairly high level of support, although the explanation of the concept differed from discussion to discussion. This option ranked third in popularity in the University town hall meeting and, in several community meetings, it ranked higher than all other options. However, its support in the Working Group Internet poll was below 50 percent.
Figure 9:
Responses to Trade-off Questions on Working Group Poll and from University Internet Town Hall Meeting
| How much do you agree or disagree with the following options
to assure coverage for all Americans? % who "Agree" or "Strongly Agree" |
Working Group Poll | University Town Hall Meeting |
| Offer uninsured Americans income tax deductions, credits, or other financial assistance to help them purchase private health insurance on their own | 42% | 35% |
| Expand state government programs for low-income people, such as Medicaid and the State Children’s Health Insurance Program, to provide coverage for more people without health insurance | 68% | 71% |
| Rely on free market competition among doctors, hospitals, other health care providers and insurance companies, rather than having government define benefits and set prices | 23% | 16% |
| Open up enrollment in national federal programs like Medicare or the federal employees’ health benefit program | 64% | 63% |
| Require businesses to offer health insurance to their employees | 56% | 47% |
| Expand neighborhood health clinics | 73% | 79% |
| Create a national health plan, financed by taxpayers, in which all Americans would get their health insurance | 70% | 78% |
| Require that all Americans enroll in basic health care coverage, either private or public | 47% | 74% |
| Increase flexibility given states in how they use federal funds (such as Medicaid and the State Children's Health Insurance Program) to maximize coverage | 55% | 58% |
| Expand current tax incentives available to employers and their employees to encourage them to offer insurance to more workers and their families | 69% | 61% |
The open-ended comments submitted to the Working Group provide some additional insight into how people view the health care system, how they want it changed, and what trade-offs they are willing to make. More than 6,000 people (6,224) wrote responses, sometimes fairly long, to the general questions on both the Internet as well as on paper forms sent to the Working Group.
In general, responses to the open ended question about paying for health care were very similar to responses to the questions regarding trade-offs and recommendations. There are comments from a small number of individuals who are strongly opposed to major changes to the current system or to any changes that would increase the government’s role in health care, but these were not the typical comments we received or what we heard in meetings or from the Internet poll.
As illustrated in Figure 10, analysis of the comments shows that when
asked about what kinds of changes should be made to the way we currently
pay for care, most wrote about the need for a single health care system.
We know from the comments submitted as well as the discussions at the
meetings that the notion of a single health care system means a number
of different things to different people. For some, the most important
issue clearly was the need for a government-run program. For others,
it was an administratively simple program that would be available to
everyone but provided in the public and private arenas. Among the 2,511
respondents who wrote about the need for a single health care system
in response to an open-ended question about how health care should be
financed, 43 percent recommended a single-payer system, while 24 percent
discussed national health care and 18 percent discussed universal health
care. The remainder discussed the ideas of universal Medicare, universal
coverage, universal basic care, or universal access.
Figure 10:
Our current way of paying for health care includes payments by individuals, employers, and government. Are there any changes you think should be made to this system?
(Working Group Comments on Open-Ended Questions)
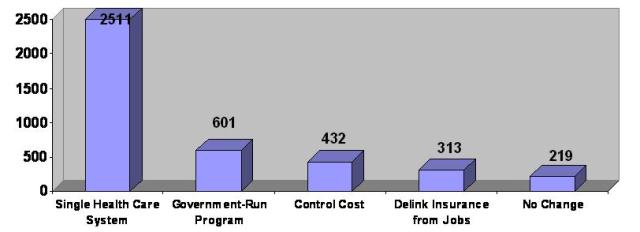
And, while a minority expressed the view that market reforms and advancements in technology could help to control costs and lead to better access to care, most of the people we heard from want more fundamental change.
The same notion—the need for a single national health care system—dominated the responses to the final question that asked people for the single most important recommendation for improving health care for all Americans. See Figure 11.
Figure 11:
What is your single most important recommendation to make to improve health care for all Americans?
(Working Group Comments on Open-Ended Questions)
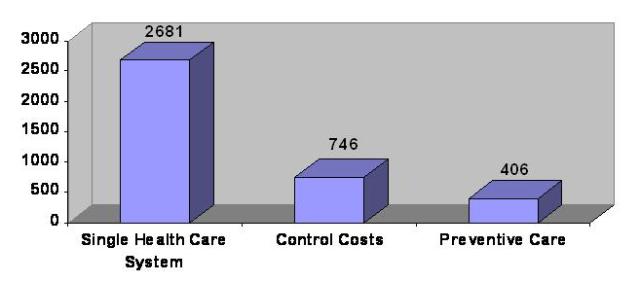
There is a great deal of diversity in the ways people envision a reformed system. They believe this can be accomplished, and most believe that the resources are already there in our current system to achieve this goal. A selection of sample comments is provided below.
The Working Group Heard Many Views about How to Make Health Care Work for All Americans: Examples
"We need a single-payer system to control costs and promote efficiency, and it has to be universal."
"I think the only thing that will work is creating a system that includes everyone at a basic level of care with significant incentives for preventive care. It could be done through a system of clinics located near grocery stores (or WalMart-type stores), in schools and community heath centers."
"Let's just do Medicare for everyone. And establish a universal standard of electronic record keeping. Then everybody can go to the doctor of their choice, when they need to, and nobody falls through the cracks. And our health care system can focus on getting the right treatment to people the best way, and the health care database can track what treatments work best for whom, in the most cost effective way. Until we have a system that guarantees universal, complete coverage, we will never be able to track what basic, effective health care really costs or establish mechanisms --or even rationing (which I don't think we need)-- that does what is best for all;"
"Everyone pays a fair share, everyone has health care benefits."
"A non-profit single payer system that covered everyone would be the best solution. This would save billions in the total cost of health care in America. This plan could buy drugs with huge bulk discounts like Medicare & congressional, & veterans plans do."
"Require all Americans to choose a health care option and allow health care choices. Then let the free market reduce the costs. The default option is a free Medicaid type program that only provides emergency and preventative care."
"I believe if Americans see that financing is more fair (rich paying more than the poor, the young contributing to the care of the elderly, the healthy paying for the sick) and all according to their level of income, this would be the first step in Americans accepting financial trade-offs. If the financing is not transparent and fair, there will be perpetual resistance. Second, I believe there must be set up a public infrastructure for setting standards of coverage and the availability of services that we are willing to fund. Such a public commission would include both citizens and representatives of all health care professions meeting apart from state or federal government. Such commission governance should be on the state, not federal, level so that local management is undergirding the system. Health resource management is local. When American citizens see that a public entity is taking the time and expertise to decide transparently what should and will be covered according to some stated ethic and philosophy of health care goals, trade-offs become more easily acceptable because the public is involved (not private corporations or remote federal agencies making such decisions). And finally, the public and local health care professionals should have the right and access to express their opinions and desires to such a public commission. There is a decision-making infrastructure that carries real authority and control but that is also permeable and open to citizen and professional input."
"All insurance should be tax deductible whether employer provided or individually purchased, as well as health expenses should be deductible below the 7.5 percent threshold. More transparency in both quality and cost so that people can truly become health care consumers. Government plans need to provide BASIC coverage and support care through community health centers as most efficient way for free care to be administered."
"I believe people should have a choice in selecting and paying for their healthcare. However, I believe the government should provide catastrophic coverage for all people. It will pay for itself in reduced neglect and dependency on government welfare and other programs."
"Put everyone in one risk pool and have a publicly financed, privately delivered system instead of paying high administrative costs for private insurance companies."
"Develop a coordinated system through the government that assures access for all, including focusing on preventive care. Health care should be regulated -- like utilities are regulated. The private sector system is not working for the US. Every other developed country has figured out a system; why can't we?"
"A single-payer system with a massive investment in information technology that provides universal access to patients as well as providers."
"Enact a single payer system of national health insurance with national standards and a global budget in which inequalities in health care delivery would be monitored and reported by race, ethnicity, income, and disability status at the state and community levels to identify inefficiencies that could be reduced by incorporating non-discrimination standards into the regulatory structure at the federal and state levels."
"We need to set up a system like Social Security, where all working people pay into it, but all get equal coverage. We also need to tax not-for-profit institutions and systems that are currently acting very much like for-profit systems to cover insurance costs for the uninsured, the elderly, and disabled. If these systems are competing with one another, and they are, they must contribute to the community need through tax dollars, since they are duplicating services and keep building facilities that are not needed."
"Medicare and the VA are and have been working. They are cheaper than other options already in place and are more efficient in administrative costs than many other options."
"A non-mandatory, semi-private, semi-government run health insurance/free (or at least affordable, possibly based on income levels) health care program to everyone in the country. A health care program completely run by the government wouldn't work, but neither would one that was privately run - something comparable in theory to the FEHBP. And it should be either free service (paid for by taxes) for the patron, or be priced according to income and possibly 'risky' behaviors."
"In addition, we need a system where health care is provided by those best able to do it most efficiently including the highest quality. There is too much reliance on physician specialists and not enough on family physicians and nurse practitioners, nurse-midwives, nurse anesthetists, etc."
"I like the idea of the health savings accounts -- but the people that need the help can't afford the cost of the high deductible insurance, so how can they afford to put $2500 or so a year in the savings portions? Paying medical expenses from an account that they manage, might make people monitor their health care costs. I do believe that people on SSI - Medicaid overuse the system. But -- how can they not. They don't have any experience with the health care system, having put off all but the most critical care all of their lives. They only know the emergency room, because they have only sought medical care in extreme emergency in the past. To make the health savings account work, I think the government should put the $2500 into the health savings account, for all individuals below a certain income level."
"Create a system that seamlessly covers individuals from birth to death. Health care is about the individual, not whether they work, or have a disability, or fall within a certain age range. We keep everything in this country piecemeal and segregated by false categorization and because of that ensure a fragmented system with lots of individuals falling through the cracks. Get rid of the fractured system based on the private market. It doesn't work. It is costly and creates too many gaps in care."
"There needs to be some combination of these things to allow coverage for all Americans. Maybe we could expand Medicare/Medicaid, or allow people without coverage to enroll in the federal employees’ plan, with a premium based on a sliding fee scale, so all pay something."
Endnotes
1 The New York Times/CBS News Poll of 1,229 adults, conducted January 20-25, 2006.
2 Employee Benefit Research Institute and Mathew Greenwald & Associates, Inc. 1998-2004 Health Confidence Surveys. “Public Attitudes on the U.S. Health Care System: Findings from the Health Confidence Survey” EBRI Issue Brief No. 275. November 2004. See Figure 5: Rating of Health Care System in America Today, 1998-2004.
3 Wall Street Journal Online/Harris Interactive Poll of 2,242 U.S. adults, conducted online by Harris Interactive September 6-12, 2005. See The Wall Street Journal Online (October 20, 2005), “Poll Shows Strong Public Support For Range of Health Practices.”
4 The New York Times/CBS News Poll of 1,229 adults, conducted January 20-25, 2006.
5 Gallup Poll of national random sample of 1,010 U.S. adults age 18+, conducted in September 2005. See The Gallup Poll (November 1, 2005), “Healthcare Panel: Costs More Troubling Than Quality.”
6 Employee Benefit Research Institute and Mathew Greenwald & Associates, Inc. 1998-2004 Health Confidence Surveys. “Public Attitudes on the U.S. Health Care System: Findings from the Health Confidence Survey” EBRI Issue Brief No. 275. November 2004. See Figure 19: Confident in Selected Aspects of the Health Care System, 2004.
7 USA Today/Kaiser Family Foundation/Harvard School of Public Health: Health Care Costs Survey (August 2005) conducted by telephone by ICR/Harvard University between April 25 and June 9, 2005, with 1,531 adults age 18 and over responding. See Chart 6: Trends in Ability to Pay for Health Care. Additional survey sources include The Gallup Organization and Pew Research Center.
8 The New York Times/CBS News Poll of 1,229 adults, conducted January 20-25, 2006.
9 The Pew Research Center for the People and The Press Poll of 1,405 U.S. adults from March 8-12, 2006. “March 2006 News Interest Index.”
10 Wall Street Journal/Harris Interactive Health-Care Poll of 2,325 U.S. adults conducted by Harris Interactive between July 11 and 13, 2006. See the Wall Street Journal Online (July 31, 2006), “Higher Premiums for Those with Unhealthy Lifestyles Supported by 53 Percent of U.S. Adults.”
11 Gallup Poll of national random sample of 1,010 U.S. adults age 18+, conducted in September 2005. See The Gallup Poll (November 22, 2005), “Healthcare Panel: More Information, Stat.”
12 Wall Street Journal Online/Harris Interactive Health-Care Poll of 2,267 U.S. adults conducted online by Harris Interactive between September 21 and 23, 2004. See The Wall Street Journal Online (October 1, 2004), “Doctors’ Interpersonal Skills Valued More than Their Training or Being Up-to-Date.”
13 Wall Street Journal/Harris Interactive Health-Care Poll of 2,325 U.S. adults conducted by Harris Interactive between July 11 and 13, 2006. See The Wall Street Journal Online (July 31, 2006), “Higher Premiums for Those with Unhealthy Lifestyles Supported by 53 Percent of U.S. Adults.”
14 Wall Street Journal/Harris Interactive Health-Care Poll of 2,325 U.S. adults conducted by Harris Interactive between July 11 and 13, 2006. See The Wall Street Journal Online (July 31, 2006), “Higher Premiums for Those with Unhealthy Lifestyles Supported by 53 Percent of U.S. Adults.”
15 Los Angeles Times/Bloomberg Press of 2,563 adults conducted by Roper Center for Public Opinion Research between February 24 and March 5, 2006.
16 Wall Street Journal Online/Harris Interactive Health-Care Poll of 2,587 U.S. adults conducted online by Harris Interactive between November 13 and 17, 2003. See The Wall Street Journal Online (December 4, 2003), “Most People Uncomfortable with Profit Motive in Health Care.”
17 Wall Street Journal Online/Harris Interactive Health Care Poll of 2,048 adults conducted online by Harris Interactive between September 30 and October 4, 2005. See The Wall Street Journal Online (October 7, 2005), “Poll Indicates Strong Support for New Medical Technologies.”
18 Harris Interactive telephone survey of 1,012 Americans age 18+ between February 8-13, 2005. See Alan F. Westin testimony at the hearing on privacy and health information technology (February 23, 2005) www.patientprivacyrights.org, under News Room.
19 Wall Street Journal Online/Harris Interactive Health-Care Poll of 2,007 U.S. adults conducted online by Harris Interactive between December 12-14, 2005. See The Wall Street Journal Online (January 6, 2006), “Kicking a Bad Habit Could Pay Off.”
20 Wall Street Journal/Harris Interactive Health-Care Poll of 2,325 U.S. adults conducted by Harris Interactive between July 11 and 13, 2006. See The Wall Street Journal Online (July 31, 2006), “Higher Premiums for Those with Unhealthy Lifestyles Supported by 53 Percent of U.S. Adults.”
21 The Pew Research Center for the People and the Press (May 10, 2005) “Beyond Red vs. Blue.” The 2005 Political Typology Survey is a national telephone interview sample of 2,000 adults age 18 and over. The Typology Callback Survey conducted in March 2005 obtained 1,090 respondents from the initial December 2004 survey. The national sample of 1,284 adults in the 2003 survey was conducted by Princeton Survey Research Associates between July 14 and August 3, 2003.
22 The New York Times/CBS News Poll of 1,229 adults, conducted January 20-25, 2006. See CBS News Online (May 13, 2004) “Poll: Economy Remains Top Priority.”
23 ABC News/Washington Post Poll, with a national sample of 1,000 adults, was conducted from October 9-13, 2003.
24 NORC at the University of Chicago survey, implemented by International Communications Research (ICR), with random sample of 2,024 respondents between August 4-10, 2004. Schur, CL, Berk, ML, and Yegian, JM. (November 10, 2004), “Public Perceptions Of Cost Containment Strategies: Mixed Signals For Managed Care.” Health Affairs Web Exclusive: W4-516 – W4-525.
25 Employee Benefit Research Institute and Mathew Greenwald & Associates, Inc. (August 9, 2005) “2005 Health Confidence Survey: Wave VIII, June 30-August 6, 2005.”
(To view documents posted on this web site as PDF files or in other formats, please read our Format help page.)