Fourteen community meetings were held during the comment period on the Working
Group’s interim recommendations, which began June 2, 2006. They varied
in size, sponsorship, and direct Working Group involvement. Three of the meetings
were formally organized by the Working Group: two public meetings in Oklahoma
City and Milwaukee, and a meeting held at the PayPal campus in San Jose, California
for employees of eBay and PayPal. The Mississippi Extension Service, out of
Mississippi State University, which earlier in the year had organized meetings
across that state, and held meetings on the interim recommendations in Jackson,
Hattiesburg, and Greenville which were facilitated by a Working Group staff
member. The Dade County Health Department and the Health Foundation of South
Florida organized a meeting in Miami that a Working Group member facilitated.
Finally, in Muncie, Indiana; Corvallis, Oregon; Cleveland, Ohio; Columbus,
Indiana; and Birmingham, Alabama, local groups organized meetings. Two meetings
were held in both Columbus and Birmingham. In all, over 700 people attended
these meetings.
While a few of these meetings used the structure of the earlier community
meetings and were organized around the four congressional questions, the vast
majority focused exclusively on the Working Group’s Interim Recommendations.
The participants in the meetings varied: attendance at some meetings was dominated
by people who work in health care. In general, as at the Working Group’s
earlier community meetings, many attendees were well-educated, middle-aged
women. The Oklahoma City meeting was notable for its over 300 participants
and diversity of views.
Public reaction to the interim recommendations from these meetings was consistent
with the messages it received on the internet and in the mail. The sentiment
among participants was that the American health care system is in trouble
and needs change. Some participants saw health care as a global issue, where
we have much to learn from other countries. In general, there was strong support
for the recommendations, individually and as a package, but a common reaction
among participants was that while they agreed with the recommendations, they
did not go far enough. A significant percentage of participants, averaging
around 20 percent at some meetings, did not support the recommendations, while
others were not sure.
At most of these meetings, there was vocal endorsement of “universal
health care,” which was often coupled with support for a single payer
system. At many meetings, there was also an articulate minority concerned
about current costs and the damage that failure to address these costs could
inflict on American competitiveness.
At many meetings participants had trouble with the recommendation proposing
protection against high health care costs and wondered why the Working Group
had this limited focus. The Working Group saw this measure as an immediate
first step toward the availability of a core set of services for all in 2012,
and has clarified both the recommendation on protection against high health
care costs and its relationship to the ultimate goal in its final report.
At the well-attended Oklahoma City meeting, the Working Group member and
staff were gratified by participants’ unexpectedly enthusiastic reaction
to two recommendations, Integrated Community Networks and Restructuring End-of-Life
Care. Each of these recommendations calls for a rethinking of the status quo
with a focus, in major part, on better integration of services at the local
level. The response in Oklahoma City suggests the reservoir of energy, imagination
and expertise that exists in communities across the country that can be brought
to bear on these two recommendations in particular.
The Working Group received over 100 comments on its Interim Recommendations
during the public comment period from organizations. Collectively these organizations
spoke on behalf of consumers, health care and other professionals, health
care organizations, business, labor, insurers, and religious groups. The city
of Philadelphia and the Cherokee Nation provided comments. David Walker, Comptroller
General of the United States, also provided comments. Several organizations
who advocate for low-income people commented, as did groups that have been
formed to pursue health system change. Some organizations provided detailed
critiques of each recommendation; others focused on one or two. Some of these
organizations represent thousands, even millions of individuals. In some cases
local chapters of organizations reiterated or expanded upon the views of their
national organization. Some organizations compared the Working Group’s
recommendations to their own established positions, sometimes enclosing documents
spelling out their views.
A summary of individual comments received from organizations follows. The
individual letters can be viewed on the Working Group’s website www.citizenshealthcare.gov.
The general response to the Working Group’s recommendations was positive,
and when organizations were critical, more often than not, it was because
the writers believed that the recommendations could have gone further. Several
organizations questioned the reordering of the recommendations that took place
on the Working Group’s website about halfway through the comment period.
In that revision of the recommendations, to make clear the sequence of implementation
steps, the Working Group made the “Guarantee Protection against Very
High Health Care Costs” its first recommendation because it could take
place relatively quickly. Commenters believed that this move led to a loss
of focus on the Working Group’s call for affordable health care for
all by 2012.
About one in four of the comments from organizations were submitted by federally-funded
Community Health Centers or state or national membership organizations representing
these centers. These comments were generally supportive of the Working Group’s
Interim Recommendations with one significant exception. These organizations
opposed the proposal to “Expand and modify the Federally Qualified Health
Center concept to accommodate other community-based health centers and practices.”
They noted that community-based, user-dominated governance has been a hallmark
of the Community Health Center program since its inception forty years ago
and a source of patient empowerment unique in the health care system which
should not be modified.
Of comments received from organizations, about one-quarter focused on advocating
for universal comprehensive health care. Some praised the Working Group’s
recommendations as a “strong call for health care coverage for all”
but more frequently commenters believed that the recommendations did not go
far enough. In all over one-fifth of the organizations commenting called for
some form of a national comprehensive tax-payer financed health care system.
Many of these commenters cited the Working Group’s polls and community
meetings to support their views and voiced the belief that the Working Group’s
recommendations did not accurately reflect public input.
In contrast to these comments, the Working Group received four comments that
were very critical of its Interim Recommendation because of the increased
emphasis they perceived in them on government’s role in health care
and lack of emphasis on market-based approaches. One of these organizations
challenged the Working Group’s findings because its public outreach
efforts did not reach “a representative cross section of the public”
and failed to capture the views of the middle class.
A number of comments were received from professional associations representing
various types of health care provider or service. In addition to making more
general comments, they often argued for adequate attention to their particular
interests, such as the health care needs of children, reproductive health,
dental health, mental health services, palliative care and HIV care.
- Community health center advocates expressed concern about expanding
and modifying the Federally Qualified Health Center concept.
- Many advocacy organizations were disappointed that the recommendations
emphasized protection from high cost care rather than access to high
quality care for all.
- These same advocacy organizations criticized the recommendations
for not going far enough in recommending universal comprehensive health
care coverage for all.
- Other groups emphasized the need for free market health care reforms
and did not support increased government involvement in health care.
- Groups representing specific populations highlighted the needs
of the people they represent and urged inclusion of provisions that
would specifically address their concerns.
- Various professional associations who work within the health care
system advised including specific health services or references to
specific providers in the recommendations.
|
| ORGANIZATION |
COMMENTS |
| Common theme: focus on integrated
community health networks |
Access to Care
Westchester, Illinois |
• Strongly agrees with community networks recommendation to broaden
the FQHC concept to include community-based health centers and programs
serving under-served populations
• Advocates consideration
of their model of care which uses private physicians in their own clinics
rather than designated public health clinics |
Numerous Community Health Centers and related organizations
(see list of commenting organizations at right following summary of comments)
|
• Expresses concern with proposal on expanding and modifying
FQHC concept
• Argues that patient-dominated health
clinic boards are a unique and important feature of the successful Community
Health Center program
• Urges retention of current
FQHC legislation and seeks independent provisions for expanding providers
in community networks
• Argues that the community networks
recommendation does not reflect the majority sentiment expressed in Working
Group community meetings
Commenting Community Health
Centers and related organizations:
Allen Hospital, Iowa Health System, Waterloo,
Iowa
Association for Utah Community Health, Salt
Lake City, Utah
Avis Goodwin Community Health Center,
Rochester, New Hampshire
Bi-State Primary Care Association,
Concord, New Hampshire
Colorado Community Health Network,
Denver, Colorado
Community Health Center of Burlington,
Inc., Burlington, Vermont
Community Health Care
Association of New York State, Albany, New York
Community
Health Center of Rutland Region, Bomoseen, Vermont
Community
Healthcare Network, New York, New York
Coos County
Family Health Services, Berlin, New Hampshire
Decatur
County Community Services, Leon, Iowa
The Georgia
Association for Primary Health Care, Decatur, Georgia
Community
Health Centers of Southern Iowa, Leon, Iowa
Hometown
Health Centers, Schenectady Family Health Services, Schenectady,
New York
Hudson River Healthcare, Peekskill, New
York
The Institute for Urban Family Health, New
York, New York
Lamprey Health Care, Newmarket,
New Hampshire
Lutheran Family Health Centers, Brooklyn,
New York
National Association of Community Health Centers,
Inc., Washington, D.C.
New Jersey Primary Care
Association, Princeton, New Jersey
Oak Orchard
Community Health Center, Brockport, New York
One
World Community Health Center, Inc., Omaha, Nebraska
Oregon
Primary Care Association, Portland, Oregon
People’s
Community Health Clinic, Waterloo, Iowa
River
Hills Community Health Center, Ottumwa, Iowa
William
Ryan Community Health Center, New York, New York
United
Community Health Center, Storm Lake, Iowa
Whitney
Young Jr. Health Services, Albany, New York |
National Assembly on School-Based Health Care
Washington, D.C. |
• Advocates for integrating school-based health care into national
health care and education systems
• Advises securing
a consistent funding stream for school health centers by authorizing school
health centers as part of the health care safety net and ensuring that
the public health insurance program reimburse SBHC services |
| Common theme: advocating for universal comprehensive
health care |
American Federation of State, County, and Municipal Employees
Washington, D.C.
|
• Argues consideration of different language in the catastrophic
coverage recommendation to prevent employers from shifting costs of mandating
insurance onto employees
• Urges Working Group fulfill
its mandate and provide a stronger endorsement of a comprehensive national
health care system to reflect the majority public opinion from community
meetings and polls
• Requests exploration of public
catastrophic coverage
• Argues that quality and efficiency
recommendation uses too broad a definition of fraud and waste, urges specifying
“fraud, waste, and abuse in the system as a whole as it relates
especially to for-profit providers of prescription drugs and health care”
• Argues that report should include explicit language to
support government’s use of purchasing and regulatory powers to
rationalize prescription drug prices and control profits of insurance
companies and other corporate entities |
Catholic Health Association of United States
Washington, D.C. |
• Strongly supports universal health care for all Americans, but must
include non-citizens as well
• Urges Working Group to define “affordable,” in relative terms
• Asks clarification of definitions of palliative, chronic, hospice, and
end-of-life care
• Advocates for explicit language in the report condemning physician-assisted
suicide |
Center for Medicare Advocacy, Inc.
Washington, D.C. |
• Advocates for a universal single payer health care system
• Asserts that high deductible coverage is only a stop gap measure and
leads to the “doughnut hole” effect |
Coalition for Democracy of Central New York
Bovina Center, New York |
• Argues that recommendations were too vague and need to include provisions
for simplifying the health care delivery and financing
• Advocates for a health care system that mirrors the Canadian one |
United States Conference of Catholic Bishops: Department of
Social Development and World Peace
Washington, D.C. |
• Praises inclusion of a strong call for universal health care coverage
with access to a core set of services and financial protection against
high health care costs
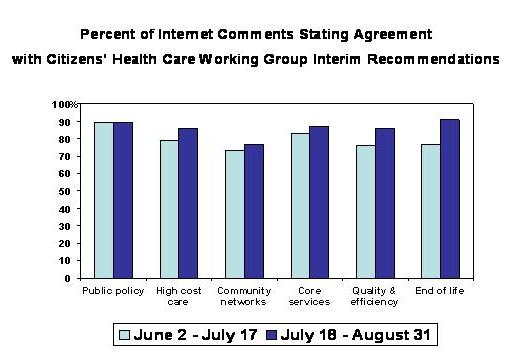
• Observes that the most striking outcome from the Working Group’s outreach
efforts is that 90 percent of the public who responded to the Internet
poll and/or participated in community meetings agreed that affordable
health care for all should be public policy
• Urges that procedures such as abortion and euthanasia, that they describe
as morally objectionable, be excluded
• Reaffirms their position that “health care is a fundamental human
right and reform of the nation’s health care system must be rooted in
values that respect human dignity, protect human life, and meet the needs…[of
the poor].” |
Family Planning Advocates
Albany, New York |
• Advocates for universal single-payer health care for all, including
non-citizens living in U.S.
• Urges Working Group to expressly advocate for comprehensive reproductive
health services
• Asserts that “affordable” health care needs to be more explicitly defined
• Argues for increasing reimbursement rates for neighborhood clinics
• Says report should explicitly address high profit margins of health
insurance companies and drug companies
• Urges inclusion of abortion services |
Health Care for All/NJ
Hoboken, New Jersey |
• Argues interim recommendations do not accurately reflect citizen
feedback from the public at community meetings
• Asserts that congressionally mandated questions were biased — leading
respondents to discuss the need for “core” rather than comprehensive coverage
• Believes recommendations should advocate explicitly for a national,
universal single-payer health care system to accurately reflect citizen
feedback |
Health Care for All/Washington
Seattle, Washington |
• Argues interim recommendations do not accurately reflect citizen
input at community meeting and advocates for comprehensive national health
care for all |
Institute of Social Medicine and Community Health
Washington, D.C. |
• Argues recommendations be revised to reflect public feedback and
advocate for a comprehensive health care package for all as soon as possible
• Supports a civil rights approach to health care processes
• Urges clarification of process for arriving at universal health care
|
International Association of Machinists and Aerospace Workers
Upper Marlboro, Maryland |
• Asserts that affordable health care for all Americans should be the
first recommendation
• Argues for adding “to not harm” to the core values and principles
section
• Asserts that core benefits package should be broadened to include comprehensive
benefits
• Urges explicitly clarifying that protection against high costs is an
incremental step toward health care for all
• Expresses concern that the public-private partnerships discussed in
the community networks recommendation will lead to for-profit entities
misusing tax dollars |
League of Women Voters Health Care Working Group
Medfield, Massachusetts |
• Urges reordering of recommendations so that public policy recommendation
is first — reflecting community feedback and support
• Argues for stronger endorsement in the report for national health care
plan, financed by taxpayers, that gives all residents equal quality of
care |
National Coalition of Mental Health Professionals and Consumers
Commack, New York |
• Advocates ensuring that mental and substance abuse services are not
relegated to a low priority in the recommendations
• Argues that the interim recommendations do not reflect public sentiment
from community meetings and poll results
• Asserts the common message was for a universal, comprehensive system
• Argues that rising costs in the health care industry come from high
prices for care, administrative costs, and too many basic services performed
in a clinical setting |
Michigan Legal Services
Detroit, Michigan |
• Asserts that focus of recommendations should shift from covering
high-cost care to providing universal comprehensive health care coverage
• Advises keeping the basic structure of federally funded health care
centers
• Argues for focus on reducing administrative costs and highlighting preventative
services and primary care and focusing on the delivery system instead
of financing |
Michigan Universal Health Care Access Network
Detroit, Michigan |
• Argues interim recommendations do not go far enough and should include
rating criteria for judging a new health care system
• Advocates for reducing health care administrative costs and inefficiencies
• Argues for financing health care through a new progressive income tax
rather than the current fragmented payment system
• Argues for a need to address how our current system decreases nation’s
global economic competitiveness
• Asserts that health care should be viewed as a public good
• Follow-up letter: Asserts frustration that recommendations
do not advocate for a progressive tax to finance publicly a national health
care program; emphasizing protection against high health care costs will
be costly and inefficient but applauds Working Group’s commitment to comprehensive
health care for all |
Midwives Alliance of North America
Fairfax, California |
• Argues that report needs to reflect citizen feedback at community
meetings and advocate for universal national, single-payer health care
for all — financed partially by taxpayers
• Agrees with promotion of evidence-based medicine, expansion of community
health clinics, and emphasis on home-based end-of-life care
• Argues for inclusion of midwifery services in core package of services
|
National Association of Free Clinics
Washington, D.C. |
• Urges inclusion of a definition of “high out of pocket costs”
• Argues that the report does not tackle non-citizens’ need for health
care
• Advocates for including vision and hearing services in the core benefits
package
• Expresses a strong need to make a distinction between free clinics and
federally funded health care centers and offers suggestions aimed specifically
at free clinics
• Argues that health care reform needs also to address potential public
health crisis crises (e.g. New Orleans after Hurricane Katrina) |
National Advocacy Center, Sisters of the Good Shepherd
Silver Spring, Maryland |
• Praises Working Group recommending affordable health care for all
Americans by 2012
• Advocates reordering the recommendations so that this recommendation
comes first |
NETWORK
Washington, D.C. |
• Advocates for affordable and accessible health care for all by 2012—calls
for a transformation in health care based on social justice |
Public Citizen
Washington, D.C. |
• Argues that Working Group needs to expressly advocate for a single-payer
system in the recommendations
• Provides arguments on benefits of single-payer national health care
model |
Philadelphia Area Committee to Defend Health Care
Philadelphia, Pennsylvania |
• Argues that interim recommendations do not reflect public sentiment
at community meetings because they do not advocate for a single payer
universal national health care system
• Urges Working Group to draft stronger recommendations that reflect majority
opinion at the community meetings |
Universal Health Care Action Network
Cleveland, Ohio |
• Divides critiques into three broad categories: how the recommendations
are framed, concern about how accurately they reflect public feedback,
and a set of comments on the feasibility of individual recommendations
• Argues that recommendations are inter-related and need to be debated
as a comprehensive reform package rather than separately
• Asserts that American health care system is not a system but is a “collection
of loosely linked systems”
• Argues that interim recommendations do not accurately reflect the majority
who provided feedback to the Working Group and asked for a national health
plan, financed by tax payers. |
Universal Health Care Action Network of Ohio
Columbus, Ohio |
• Advocates for changing the order of the recommendations so that Affordable
Health Care for all recommendation comes first
• Argues that protection against high health care costs should be broadened
to include nominal costs for low income persons
• Asserts that integrated community health networks should be available
to all
• Urges more aggressive measures to curtail waste
• Argues for eliminating tax cuts for the wealthy |
Reach Out America
Great Neck, New York |
• Disagrees with protection against high health care costs, affordable
health care, and a core benefits package in lieu of a universal, publicly
financed system of health care |
RESULTS
Washington, D.C. |
• Advocates reordering recommendations to place affordable health care
for all as number one
• Argues that the timeline needs to be added to spur Congress and the
Executive Branch to act |
The Workmen’s Circle
New York, New York |
• Disagrees with the revised order of the recommendations and advocates
for retaining affordable health care for all as the first recommendation
• Argues that the integrated community health network recommendation fails
to address the current two-tier system of health care
• Disagrees with including “core” benefits package and protection against
high health care cost recommendations as they deflects from the ultimate
goal of providing comprehensive health care for all |
Washington State Ad-Hoc Coalition on the Citizens Health Care
Working Group
|
• Urges shortening the Values and Principles section to the first three
bullets
• Argues first recommendation should be “It should be public policy
that all Americans have affordable health care”
• Advocates second recommendation should read, “There should be a
national health plan, financed by taxpayers, in which all Americans would
get their health insurances”
• Argues third recommendation should read, “A sufficiently comprehensive
benefits packages for all Americans should be defined”
• Proposes additional changes to other recommendations
• Follow up letter: argues for removing “core”
and replacing it with “comprehensive” benefit package
• Advocates for not allowing insurance companies and employers to be decision
makers in creating the core benefits package
• Reiterates Working Group should advocate for comprehensive health care
in response to public response through surveys and community meetings
|
| Common theme: Promote a free market health care
system |
Association of American Physicians and Surgeons
Tucson, Arizona |
• Disagrees with the interim recommendations in favor of private market
approaches and believes that universal coverage leads to restricted access
to care |
ERISA Industry Committee
Washington, D.C. |
• Argues that Working Group should differentiate health care from health
insurance arguing that Americans already have access to free health care
• Asserts that free health care insurance for all would place an undue
burden on taxpayers and lead to rationing
• Asserts that a tax-payer system will lead to moral hazard
• Argues for restricting unnecessary medical liability lawsuits
• Urges Working Group to promote incentives for providers who provide
high quality and efficient care |
Health Care America
Washington, D.C. |
• Asserts that the Working Group report is not practical because it
does not discuss how to implement the recommendations
• Argues that report implicitly calls for increase in the government’s
role in national health care coupled with a tax increase, which they assert
most Americans do not support
• Suggests community meetings failed to capture a representative sample
of America’s middle class
• Argues that greater health care coverage does not imply greater access
to care
• Supports market competition between health plans and packages as the
best approach for consumers to enjoy choice in health care
• Advocates for four solutions to limit increases in health care costs,
including: redirecting non-emergency care to more appropriate locations,
enacting medical liability reform, encouraging electronic health records,
and introducing pay-for-performance incentives to reward providers for
high quality services
• Argues that recommendation for integrated community health networks
is not notably different from the current system |
Institute for Health Freedom
Washington, D.C. |
• Uses Medicare as a case study to argue that universal, single-payer
national health care is not effective in improving health indicators,
poverty rates, provider choice, and health privacy |
| Common theme: all have a special focus |
American Academy of Actuaries
Washington, D.C. |
• Asks the Working Group refer to their publications as resources for
information on a variety of health care issues
• Special focus:: Argues that actuaries provide unique
expertise and perspective on issues related to risk and contingent events |
American Academy of Pediatrics
Elk Grove Village, Illinois |
• Special focus:: Focus on unique health needs of children
• Advocates for increasing Medicaid reimbursements for pediatric services
• Argues that integrated community networks recommendation should explicitly
refer to children and promote the “child medical home”
• Urges development of specific pediatric care quality measures |
American Chiropractic Association
Arlington, Virginia |
• Concludes that health care system needs to shift focus from caring
for the seriously ill to disease prevention, early disease detection,
and positive lifestyle changes
• Special focus: Argues chiropractic care is a major component
of efficient quality health care and should be fully integrated into the
medical delivery system |
American Dental Association
Washington, D.C. |
• Strongly supports inclusion of dental services in definition of core
health services
• Special focus: Argues oral health is an important component
of health |
American Hospital Association
Washington, D.C. |
• Presents results from its own independent “listening sessions” held
to discuss health care reform with key stakeholders resulting in 10 principles
that typify what healthcare should be in America.
• Special focus: Concludes its vision of health care reform
is parallel to the Working Group’s interim recommendations |
American Psychological Association
Washington, D.C. |
• Special focus: Concerned that the core benefits package
will not include adequate mental health services
• Argues that “evidence-base care” in benefits section needs to reflect
different diagnostic approach for mental health services
• Recommends replacing the term “medical” with “clinical” to be more inclusive
in treatment by both physicians and non-physicians |
Association of Clinicians for the Underserved
Tysons Corner, Virginia |
• Special focus: Advocates for health care reforms that
increase underserved community access to care
• Encourages greater financial incentives for clinicians to provide preventative
care and health education services |
Ascension Health
Saint Louis, Missouri |
• Special focus: Praises recommendations and provides
a strong endorsement for affordable health care, integrated community
health networks, and restructuring end-of-life care |
Seton Healthcare Network
Austin, Texas |
• Special focus: Reiterates Ascension Health’s comments |
Associations of Professional Chaplains
Schaumburg, Illinois |
• Special focus: Argues for greater emphasis on mental,
emotional, and spiritual health elements of health care |
California Pan-Ethnic Health Network
Oakland, California |
• Encourages Working Group to add a new recommendation addressing racial
disparities in health
• Special focus: Endorses recommendations but argues for
greater emphasis on communities of color |
Catholics for a Free Choice
Washington, D.C. |
• Concurs with finding that the health care system is in desperate need
of overhaul
• Special focus: Argues that core benefits package should
include services and medicines based on the needs of the patient not the
ideological beliefs of the hospital or provider |
Cherokee Nation
Tahlequah, Oklahoma |
• Argues that the unique relationships with tribes must be honored,
Indian Health Service, Tribal Programs, and Urban Indian Clinics (I/T/U)
system remain intact and federal funds be used to cover health care expenses
imposed on eligible American Indians and Alaskan Natives
• Advocates that community health networks include health care services
for Indian country
• Argues that the I/T/U system should be a critical focus in a new initiative
to improve quality and efficiency
• Special focus:: Carefully take into account how proposed
health care reforms will impact the current American Indian and Alaska
Native health care system and ensure that any changes have a positive
effect on Native Americans and Alaskan Natives |
Clinical Social Work Association
Seattle, Washington |
• Special focus: Argues to include physical, mental,
dental services in the defined core benefits package |
Clinical Social Work Guild
Arlington, Virginia |
• Special focus: Advocates for benefits parity for mental
and physical services and incorporating language that emphasizes importance
of psychosocial aspects of mental and physical health |
Congreso de Latinos Unidos
Philadelphia, Pennsylvania |
• Special focus: Argues community-based organizations
should be considered as potential outpatient and health and wellness providers/educators
especially in communities that frequently encounter obstacles to health
care due to language and cultural barriers |
Consumers Union
Washington, D.C. |
• Praises interim recommendations
• Special focus: Emphasizes need for evidence-based medicine |
End-of-Life Nursing Education Consortium
Washington, D.C. |
• Special focus: Suggests integrating end-of-life and
palliative care issues throughout all recommendations rather than addressing
the issue in a separate recommendation |
HIV Medicare and Medicaid Working Group
On behalf of 32 organizations from across the country |
• Argues that the “core” benefits package should meet the needs of people
living with HIV and AIDS
• Advocates for explicit measures to protect against high cost out-of-pocket
expenses
• Strongly supports integrating health networks, including HIV centers
of excellence, and ensuring patients have more choice over their end-of-life
care, treatment, and environment
• Special focus: Strongly supports the CHCWG interim recommendations
and its call for all Americans regardless of income to have affordable
and comprehensive health care |
Lourdes (Ascension Health)
Binghamton, New York |
• Special focus: Suggests clarifying high cost in relation
to income, otherwise generally supports the recommendations |
National Athletic Trainers’ Association
Dallas, Texas |
• Special focus: Advocates for supporting policies that
enhance injury and illness prevention and preventative care
• Argues for policies that address the shortage of health care workers
|
National Association of Dental Plans
Dallas, Texas |
• Special focus: Argues dental benefits companies are
the most effective entities to provide dental coverage with input from
dental providers |
National Association of Health Underwriters
Arlington, Virginia |
• Advises Working Group to address high health care costs with the private
marketplace subsidizing individual policies and increasing federal subsidies
for high risk pools
• Urges Working Group to encourage Americans to purchase long term care
insurance in their report
• Special focus: Advocates for retaining the national
private health care insurance market |
National Association of REALTORS
Washington, D.C. |
• Special focus: Urges support for federal legislation
that would authorize the creation of small business health plans through
trade organizations
• Suggests the small business community be represented on any independent,
non-partisan, private-public group called for in the final report |
National Committee for Quality Assurance
Washington, D.C. |
• Recommends supporting pay-for-performance programs for prevention
and chronic conditions
• Supports recommendation that enhances patient education opportunities
• Recommends making organizations who provide the core benefits package
responsible for measuring and reporting quality measures
• Special focus: Supports recommendation on improving
quality and efficiency in health care |
National Consensus Project for Quality Palliative Care
Pittsburgh, Pennsylvania |
• Argues that palliative care should be explicitly included as a core
benefit
• Urges health care policymakers to focus more attention on palliative
care to ensure higher quality and more efficiently in care
• Special focus: Advocates for placing greater emphasis
on palliative care |
Planned Parenthood Federation of America
New York, New York |
• Special focus: Advocates for CHCWG to address the
need to increase funding for public programs that provide low-income women
with comprehensive reproductive health services, as well as pre- and post-natal
care services |
Provena Central Illinois Region
United Samaritans Med. Ctr., Danville, Illinois; and Covenant Med. Ctr.,
Urbana, Illinois |
• Special focus: Supports recommendations to provide
protection against high health care costs, making affordable health care
public policy, and reforming end-of-life care to support the wishes of
the patient |
Providence Hospital (Ascension Health)
Mobile, Alabama |
• Special focus: Generally supports recommendations |
Religious Coalition for Reproductive Choice
Washington, D.C. |
• Special focus: Concerned that the content of the core
benefit package may be determined by ideological factors and not respect
diverse beliefs
• Argues for addressing the inequities in medical care and coverage within
the system
• Advocates for including comprehensive reproductive services and pre-post
natal care in the core benefits package |
St. Vincent Health (Ascension Health)
Indianapolis, Indiana |
• Special focus: Praises recommendations, placing particular
emphasis on protection against high health care costs, integrated community
health networks, and improving the quality of care |
Supportive Care Coalition
Portland, Oregon |
• Concerned that emphasis on preventative care will force Americans
living with chronic illness to be fully responsible for their own care
• Advises the CHCWG to include spiritual and bereavement services in core
benefits package
• Special focus: Urges CHCWG to integrate end-of-life
services into the other recommendations, where appropriate |
United University Church
Los Angeles, California |
• Special focus: Concerned that delivery of controversial
core services such as HIV prevention education, abortion, emergency contraception,
condom distribution will be hindered at faith-based medical facilities
|
Vista Care
Scottsdale, Arizona |
• Special focus: Agrees wholeheartedly with recommendations,
especially end-of-life |
| Common theme: Comprehensive comments on recommendations |
American Academy of Physician Assistants (AAPA)
Alexandria, Virginia |
• Supports health care delivered by qualified providers in physician-lead
teams that are accountable to high professional standards
• Advocates for incentives to control costs through optimal use of primary
care (e.g. health promotion and disease prevention), reducing administrative
costs, eliminate cost shifting, and creating greater incentives for providers
to give patients appropriate care
• Argues that fair and comprehensive medical liability reform is needed
• Endorses system reform that enhances the patient-provider relationship—
and when appropriate—defer to the patient’s family to make decisions regarding
patient care |
American College of Physicians
Washington, D.C. |
• Agrees with recommendations on moving toward universal access to care,
creating a non-partisan, public-private group to create the core benefits
package
• Argues for the need to identify target populations that are the most
in need of health care coverage, access, and care
• Urges inclusion of explicit language on how to make prescription drugs
more affordable
• Emphasizes need to make reimbursement levels for covered services fair
and appropriate
• Argues for including explicit provisions on eliminating disparities
in health care based on social, ethnic, racial, gender, sexual orientation
and demographic differences
• Advocates for stronger emphasis on basic consumer protection rights,
including rights to information
• Argues for ongoing evaluations of health care reforms
• Asserts need to respect individual choice of providers |
AFL-CIO
Washington, D.C. |
• Strongly supports end-of-life, integrated community networks, and
public policy recommendations
• Argues that $4,000 deductible for high health care cost protection is
still too high for poor Americans and would discourage necessary care
• Advocates for stronger language on greater transparency for insurance
“purchasers” not just “consumers”
• Argues for quality and efficiency recommendation to endorse payment
systems to reward high quality care and improvements in care”
• Strongly endorses the core benefits package and argues the recommendation
is in contrast to the model of care implicit in the high deductible plan |
American Medical Association
Chicago, Illinois |
• Argues that the best method of expanding health care coverage is to
cap or revoke the subsidy of employment-based coverage with the addition
of a federal tax credit or premium subsidy for the uninsured
• Supports legislation to allow individuals to “buy in” to state employee
purchasing pools
• Argues that emphasis on safety net in community health networks recommendation
will undermine proposal to expand coverage to the uninsured
• Supports price transparency, health information technology improvements
and a greater emphasis on community-based and home health alternatives
for end-of-life and long term care
• Disagrees with defining a core benefit package and instead argues that
benefit mandates should be minimized to allow markets to permit a wide
choice of coverage options |
American Medical Student Association
Reston, Virginia |
• Asserts that recommendations would be strengthened if they included
financial and long-term outcome projections
• Argues that high cost recommendation implies every American needs catastrophic
coverage, when what they need is comprehensive care including the preventative
and chronic care management health care service noted in the community
network recommendation
• Argues that if federally funded health care centers are expanded to
include new providers, they should be required to meet current federal
guidelines
• Advocates for including all providers—not just federally subsidized
programs—in provisions to improve quality and efficiency and increasing
Medicare funding to address demographic changes in aging
• Advocates for single payer system to finance comprehensive national
health care
• Stresses that the core benefits package recommendation must include
a continuing evaluation component to review/revise benefits as necessary |
American Nurses Association
Silver Spring, Maryland |
• Praises Working Group support for affordable, quality health care
for all
• Urges acknowledgement of discrepancies between community meeting input
and the recommendations
• Argues the recommendations should have more explicit language on health
care as a right for all—citizens and residents
• Advocates including more explicit language on controlling long term
costs through emphasis on primary care and health maintenance
• Asks CHCWG to clarify whether protection against high care costs includes
long term care
• Asserts that the community health networks need to be integrated with
social services
• Advises against consumer-driven healthcare because of underlying assumption
that patients are able to make the appropriate medical choices
• Urges integration of end-of-life services throughout the recommendations
• Advocates for explicit language on chronic pain management within section
on palliative care
• Asks recommendation on affordable health care policy to include language
on “removing financial barriers to care”
• Requests the CHCWG make a clear distinction between health services
and health insurance
• Advocates including specific mention of “single payer” as a preferred
path to financing reform
• Requests that insurers not play a role in defining the core benefits
package as reflected in public feedback |
American Osteopathic Association
Washington, D.C. |
• Advocates for the creation of a national data bank that evaluates
adverse medical events to improve quality of healthcare
• Advocates for focusing more on long-term impact of medical interventions
on the patient’s quality of life as opposed to controlling costs
• Disagrees with the core benefits package, arguing it is not feasible |
American Public Health Association
Washington, D.C. |
• Advocates for guaranteeing basic health coverage rather than protection
against very high health care costs
• Stresses including guaranteed Medicaid funding to federally funded health
care centers in integrated community network recommendation
• Recommends changing current Medicare payment policy for hospice care
• Argues that data and specific details are needed to support the recommendation
on affordable health care
• Requests more specifics on expert group who establishes core benefit
package |
Cincinnati USA Regional Chamber
Cincinnati, Ohio |
• Urges CHCWG to quantify affordable health care and clarify who is
calling for this recommendation
• Argues for more explicit language for each of the recommendations |
City of Philadelphia
Department of Public Health
And additional letter endorsed by 17 organizations and 39 individuals |
• Argues highlighting the importance of state and local government,
business and labor, faith-based groups, payer organizations, and representatives
for the public in defining a core benefits package
• Suggests using Philadelphia’s Health Leadership Partnership (HLP) as
a model for building and integrating community health networks
• Second letter: Reiterates City’s support of community networks recommendation
and urges use of HLP as a national model |
General Accountability Office (GAO)
Washington, D.C. |
• Urges Working Group to explicitly explain their method of incorporating
public feedback and expert opinion when developing recommendations
• Critiques public policy recommendation for not addressing implicit fiscal
challenge of charge
• Argues that recommendations need to make clear whether core benefits
package will replace Medicare and Medicaid
• Advocates for separating the core benefit package into two levels of
benefits—one universal, government basic coverage (preventative, some
wellness, and catastrophic coverage) and the other— supplemental, private
insurance to cover non-essential services
• Argues for using Medicare/Medicaid as explicit “prototypes” when promoting
affordable health care
• Advocates for establishing national ‘medical best practices’ |
Health Care Leadership Council
Washington, D.C. |
• Encourages greater emphasis on consumer education and outreach
• Advocates for government-financed private sector health Information
technology investment to spur innovation
• Encourages Working Group to argue for medical liability reforms |
Independent Living Resource Center San Francisco
San Francisco, California |
• Disagrees with any recommendation using income as a determinant policy
because that promotes a two-tiered system
• Concerned that the public/private partnerships discussed in the community
networks recommendation will lead to corrupt and wasteful government contracts
• Proposes offering free tuition in exchange for M.D.s working in low
resource locations
• Argues that greater emphasis in the report needs to be placed on independent
living for people with disabilities
• Argues that consumers need options in a core benefits package that fit
their needs |
Mid-Valley Health Care Advocates
Corvallis, Oregon |
• Urges recommendations to emphasize protection from high health care
costs for all citizens, not just low-income families
• Disagrees with new order of recommendations
• Concerned that the integrated community network will create a two-tiered
system of healthcare |
National Coalition on Health Care
Washington, D.C. |
• Advocates for inclusion of language specifying all Americans should
have access to health care insurance and timely access to care
• Argues that rising healthcare costs need to be reduced to the annual
increase in GDP per capita through limits on increases in insurance premiums
for core benefit coverage and rates for reimbursing providers
• Supports a $1 billion federal investment in improving national health
care quality and efficiency
• Urges combining high cost care and affordable health care for all recommendations
into one |
National Health Law Program
Los Angeles, California |
• Advocates for clarifying values and principles, explaining how the
recommendations will be implemented, and resolving potential inconsistencies
between the terms “medically” effective and “evidence-based”
• Supports inclusion of comprehensive women’s health and language services
• Urges recommendation to protect low-income individuals during the transition
to health care reform
• Advocates for broadly defining the standards and evidence that will
be acceptable to determine core benefits
• Argues for a financing system in which the government is the single
payer
• Advocates for financing strategies that consider low-income individuals’
existing tax contributions and relative burdens
• Urges replacement of all references to “citizens” with “Americans” with
“Americans” defined to include immigrants
• Argues that report should state that health is a human right
• Advocates for spending what is necessary to attain the highest standard
of health for everyone
• Asks for clarification that “right care at the right time” means that
low-income individuals can receive medically necessary services at no
cost without delay without cost-sharing
• Urges a distinction between “define set of benefits” and the “set of
core health services”
• Argues that recommendations should explicitly state coverage of health
service will not be linked to health status or behavior
• Suggests adding “quality” to the principle of affordability to guarantee
“quality, affordable health care coverage”
• Urges clarification of the appointment process for the private-public
group to minimize political influences
• Argues for coupling the proposal to expand health centers with the commitment
to provide sufficient resources for the task
• Advocates for maintaining the requirement that patients occupy a majority
of seats on an organization’s governing board as a condition of Federal
funding
• Suggests the Working Group define length and scope of end-of-life services
expansively with full funding by the federal government
• Argues for prioritizing the collection of racial, ethnic, and language
data as the new health information systems are implemented |
National Small Business Association
Washington, D.C. |
• Argues for requiring that everyone have healthcare coverage and providing
federal subsidies for low income individuals and
• Advocates for pay for performance incentives for health care providers
based on outcomes rather than procedures
• Suggests the individual tax exclusion for health insurance coverage
should be limited to the value of a basic benefits package
• Argues health services to be added to the core benefits package undergo
cost/benefit analysis |
Schuylkill Alliance for Health Care Access, Inc.
Pottsville, Pennsylvania |
• Advocates for patient incentives to induce healthier lifestyles
• Argues patient out-of-pocket expenses should be based on a sliding scale
• Advises using sin taxes for financing
• Argues government health agencies need to improve coordination |
Service Employees International Union
Washington, D.C. |
• Asserts importance of retaining 2012 timeline for implementing recommendations
• Argues that more attention in the recommendations needs to be given
to protecting Americans from high health care costs
• Advocates for including preventative services, long term care, and provider
choice in the core benefits package |