Table of Contents
RECOMMENDATIONS
Recommendation 1: Establish Public Policy that All Americans Have Affordable Health Care
Recommendation 2: Guarantee Financial Protection Against Very High Health Care Costs
Recommendation 3: Foster Innovative Integrated Community Health Networks
Recommendation 4: Define Core Benefits and Services for All Americans
Recommendation 5: Promote Efforts to Improve Quality of Care and Efficiency
Recommendation 6: Fundamentally Restructure the Way End-of-Life Services are Financed and Provided
PAYING FOR HEALTH CARE FOR ALL AMERICANS
An American Dialogue
Bipartisan legislation created the Citizens’ Health Care Working Group to go to the American people, to explore their values and aspirations for the American health care system, and to bring their ideas and energy for health reform back to Washington.
A Working Group as Diverse as America
Appointed by the Comptroller General of the United States, the Citizens’ Health Care Working Group is a nonpartisan body made up of 14 citizens plus the Secretary of Health and Human Services – all from very different backgrounds, experiences within the health care system, and communities across the nation. A complete list of members is available at the end of this report.
Charged to Open a Discussion
Enacted in the Medicare Prescription Drug, Improvement and Modernization Act of 2003, section 1014, the Citizens’ Health Care Working Group was charged to open a discussion about health care for every American and to “engage in an informed national public debate to make choices about the services they want covered, what health care coverage they want, and how they are willing to pay for coverage.” More specifically, the statute requested that the following questions be addressed:
-
What health care benefits and services should be provided?
-
How does the American public want health care delivered?
-
How should health care coverage be financed?
-
What trade-offs are the American public willing to make in either benefits or financing to ensure access to affordable, high quality health care coverage and services?
Following six regional hearings held in 2005 with experts, stakeholders, scholars, and public officials, the Working Group issued a report entitled The Health Report to the American People, to enable the American public to become informed participants in a national debate on health care reform. The Working Group then began its conversations across America.
| How the Working Group did its work: Community forums Over 28,000 citizen responses via the Internet One-on-one discussions in personal encounters with individual Americans Individual essays and stories Blogs, message boards and other on-line dialogue Research, including a review of all national polls from 2002 - 2006 Expert hearings Media coverage Internet message boards |
Overall, this public dialogue required an extraordinary breadth of effort to reach out to diverse communities representing a full spectrum of the American public. Working Group members participated in discussions ranging from one-on-one conversations and community meetings, to expert research and mass communications through the Internet and press. For nearly eighteen months, the Working Group engaged America through town-hall meetings, thousands of Internet communications, hearings with experts, analysis of national polls and personal face-to-face conversations, including many deliberations among the Working Group members themselves. In turn, these efforts attracted unsolicited essays, an extensive array of written comments and other communications. The Working Group carefully reviewed public input and available literature employing an inclusive, transparent, and accessible process.
Following the drafting of initial recommendations based on accumulated public and expert input, the Working Group issued Interim Recommendations which were made available for a 90-day comment period which ended on August 31, 2006. More than 6,000 individuals responded and over 100 organizations, representing millions of Americans, issued formal statements in response to these recommendations.
Outlining Broad-Based Change in American Health Care
The American people spoke about creating health care that works for everyone with remarkable consistency. Across many communities the views we heard based on community meetings, the Internet polls, and national polls formed the basis for the recommendations in this report. The Working Group does not claim to know, with complete certainty, the health care values and preferences of all Americans. Rather, deliberations were based on a careful assessment of input from many sources taking into account the gaps or biases that may be reflected in each type of information obtained.
The report that follows is a product of all these efforts – a product that is being presented to the President and United States Congress, where five committees will hold hearings.
The final recommendations from the Working Group outline both a vision and a plan for achieving broad-based change in the delivery and financing of health care in America. The Citizens’ Health Care Working Group recognizes that the issues involved are complex and challenging, and that it will take time, technical expertise and, especially, a great deal of political will to implement these strategies. The American people, who have called for these changes, will, in the end, be the ones to sustain this new vision.
For more information on the findings of the Citizens’ Health Care Working Group, visit www.CitizensHealthCare.gov.
Values and Principles
The Citizens’ Health Care Working Group believes that reform of the health care system should be guided by principles that reflect the values of the American people. In community meetings across the nation, the following principles were identified as important to most Americans:
-
Health and health care are fundamental to the well-being and security of the American people.
-
Health care is a shared social responsibility. This is defined as, on the one hand, the nation’s or community’s responsibility for the health and security of its people and, on the other hand, the individual’s responsibility to be a good steward of health care resources.
-
All Americans should have access to a set of core health care services across the continuum of care that includes wellness and preventive services. This defined set of benefits should be guaranteed for all, across their lifespan, in a simple and seamless manner. These benefits should be portable and independent of health status, working status, age, income or other categorical factors that might otherwise affect health-insurance status.
-
Health care spending needs to be considered in the context of other societal needs and responsibilities. Because resources for health care spending are not unlimited, the efficient use of public and private resources is critical.
Summary
Health Care that Works for All Americans
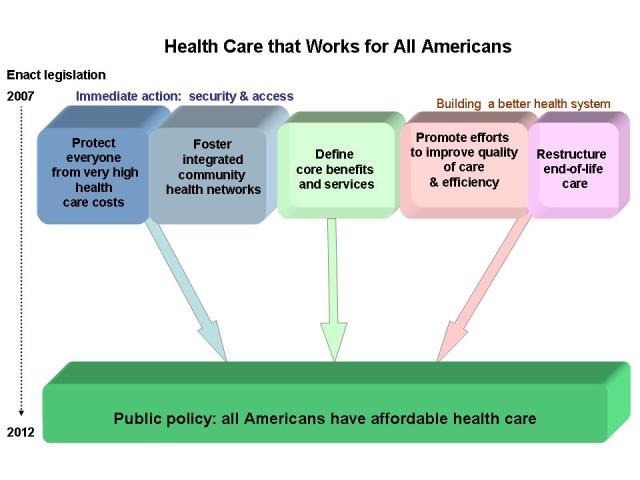
These recommendations reflect a desire by an overwhelming majority of Americans that everyone has access to affordable, appropriate health care by an established date in the not-too-distant future--2012. Encompassed in this goal is the need to make changes in the current health care system to expand access to care for those who need it as well as to improve outcomes and increase the value for money spent.
The Working Group is proposing six recommendations – organized into three sets and one overarching goal – as the forces for change. Commencing immediately, these recommendations will guide a five-year transition in American health care. The first set addresses serious threats to health security – very high costs and gaps in access to basic health care, preventive services, and health education at the community level. The second defines a package of core benefits and services, reflecting evidence-based practices and the principle of shared responsibility. The third builds a better health care system by achieving greater efficiency, improving quality, and restructuring end-of-life care.
Achieving Health Care that Works for All by 2012
Within these three sets, the Working Group recommends five multi-step actions for accomplishing its central goal stated in Recommendation 1, that “It Should Be Public Policy that All Americans Have Affordable Health Care" and that all Americans have access to a set of affordable and appropriate core health care services by the year 2012.
Initiating the work encompassed by these sets of supporting recommendations simultaneously will enable the American health care delivery and financing system to move toward achieving the broader imperative voiced by the American public.
ONE: Immediate Action to Improve Security and Access
Guarantee Financial Protection Against Very High Health Care Costs
By establishing protection against very high medical costs for all, the Working Group’s Recommendation 2 responds to two major messages from the American people. First, people believe that no one should be financially ruined by health care costs. Further, there was overwhelming public support for a new dynamic in American health care where everyone is protected, not just select portions of the population. This Recommendation can be implemented in the short term and provide a basic level of financial protection to those who do not already possess this coverage. Building this system will provide some level of immediate protection for everyone, and also has the potential to stabilize existing employer-based health insurance markets and expand the private individual and small group health insurance markets to more Americans. More important, it will provide the foundation for providing core benefits and services to all Americans called for in Recommendation 1.
Innovative Integrated Community Health Networks
Coupled with this high-cost protection, Recommendation 3 calls for bringing together national leadership and best practices with local know-how to foster innovative, integrated community health networks. This piece of health care reform draws on America’s ability to think “globally” but act “locally.” These networks will be better suited to coordinate federal, state, and local resources, improving the capacity of existing community health programs to deliver basic care and provide health promotion and education services. The combination of strong and caring community networks with innovations in quality and efficiency is key to making affordable health care available for all by 2012.
TWO: Define Core Benefits and Services for All Americans
Recommendation 4 calls for establishing an independent, nonpartisan group to begin the work of defining benefits and services that would be the standard for all Americans. This is perhaps the most challenging component of the strategy the Working Group is recommending. Identifying these core benefits through a transparent, evidence-based process, with consumer participation, can help to make all health care more effective and control health care costs. The group making these decisions would be established as a public/private entity to insulate it from both political and financial influence. It would also be an ongoing entity with stable funding, to guarantee its independence and to ensure that the benefit package continues to be responsive to evolving medical knowledge and practice.
THREE: Build a Better Health Care System
Promote Efforts to Improve Quality of Care and Efficiency
Recommendation 5 centers on how America can do a better job with the two trillion dollars spent every year on health by achieving greater efficiency and improving quality. Building on innovative strategies from both the marketplace and government to improve the quality and efficiency of the health care system and enhance the ability of individuals to receive high quality care will help to control health care costs. To date, most early successes have come in integrated delivery systems which have the concentrated resources and organizational structures to address waste and inefficiency. These resources and efforts should grow with implementation of the integrated community networks described above. The federal government, as a dominant purchaser of health care, has the ability to play a significant leadership role in promoting research and the development, demonstration, and dissemination of quality improvement efforts.
Fundamentally Restructure End-of-Life Care
As a part of improving the health care system and in response to the issue being raised persistently by the public, Recommendation 6 addresses the need to restructure end-of-life care. The American health care system must find ways to help individuals, families, and health care professionals deal with complex medical and supportive care needs more effectively by improving access to more appropriate and better care at the end of life. The Working Group acknowledges that end-of-life issues are often difficult, painful, complicated, and thus not conducive to quick or easy fixes. This recommendation seeks to better define, communicate, and make available at individual, family, community, and societal levels the support needed and wanted for one’s last days.
Proposed Financing
Implementing these recommendations requires considering how to pay for them. There may be important opportunities to reallocate existing funds spent by state and federal governments. In addition, some of the actions proposed here may yield savings to the health care system in the long term, although it is unlikely that health system improvements will yield sufficient savings over the next few years to pay for the immediate actions recommended. In response to the potential need for new resources, the Working Group has identified principles which any new funding source should meet and offers examples of options which are currently part of the national policy debate and meet these criteria.
| More detailed information, including background on the state of health care in America, analysis from the community meetings, comments and opinions provided to the Working Group, and relevant data from national polls and surveys, is reported in Dialogue With the American People and The Report to the American People (revised 2006). |
1. Establish Public Policy that All Americans Have Affordable Health Care
-
Americans should have a health care system in which everyone participates, regardless of their financial resources or health status, with benefits that are sufficiently comprehensive to provide access to appropriate, high-quality care without endangering individual or family financial security.
-
This public policy should be established immediately and implemented by 2012.
Context
In the discussion of underlying values and perceptions that began each community meeting, 94 percent of all participants agreed with the statement, “It should be public policy [written in law] that all Americans have affordable health care.” Additionally, most respondents to the Working Group’s Internet poll strongly agreed (80 percent) or agreed (12 percent) with that statement. People at many of the community meetings expressed the desire for “cradle to grave” access to health care, guaranteed in law.
A clear majority of participants preferred that all Americans receive health care coverage for a defined level of services. Currently, heath coverage – whether one has it and what is covered – depends on various characteristics, such as age or employment status. Between 68 and 98 percent of participants at the community meetings said that some defined level of services should be provided for everyone. In the Working Group’s Internet poll, 85 percent of participants also opted for a defined level of services for everyone. These findings are consistent with national polls conducted that show a clear majority expressing the view that all Americans should have health insurance. For example, a national poll conducted in September 2005 found that 75 percent of U.S. adults strongly favored (52 percent) or somewhat favored (23 percent) health insurance that covers all Americans.
Americans Share Their Vision of a New System
Americans clearly want a system that guarantees health care for everyone. The most important considerations expressed focused on people having access to affordable health care and on coverage being reliable and secure.
In addition to reliable, affordable care, people want a system in which everyone is covered for most health care costs. They want a plan that, unlike many existing health insurance plans, cannot be cancelled or lost because of a change in employment status, be priced at unaffordable levels, or exclude those with pre-existing health conditions or ongoing health problems. This health care system would provide coverage for treatment of illness and injury, as well as preventive and palliative care.
Many Americans want to choose their health care providers and be able to communicate openly with them so that they can make good decisions about their care. They also believe that a simpler, more seamless system could provide coverage to everyone more efficiently than the current system.
The implications of this vision for a new health care system are very important: Many Americans hold the view that public policy aimed at the growing crisis in health care costs cannot succeed unless all Americans are able to get the health care they need when they need it, and that all Americans pay their fair share.
Defining a Comprehensive National System
The Working Group heard from people supporting a wide variety of approaches ranging from enhanced free market choice to a totally public program as a way to ensure access to health care. A clear majority of Americans are in favor of a national policy ensuring universal coverage. However, “universal coverage” means different things to different people.
Some of the approaches advocated could be administered by private sector health plans, others could be organized through employer-sponsored coverage in the group market, and others could be run directly by the government. Many cited Medicare or the Federal Employees Health Benefits Program as models for a national system. Some identified the Veterans Health Administration (VA) system as another possible model, while others suggested that existing large integrated private health care systems could provide the best models. People pointed to these programs not only as examples of how to provide coverage, but also as systems that can better control costs and provide the infrastructure and resources needed to improve the quality and efficiency of health care delivery.
In addition to reflecting on existing systems in America, people who attended the community meetings frequently asked why other nations could provide universal coverage and still spend less per capita on health care while producing higher quality and better health for their citizens. They called attention to the strengths of these systems and many talked about their own positive experiences with a foreign health care system. Other participants pointed to problems to avoid within health care systems of other nations such as the lack of provider choice. For many, difficulties with cost and access to health care in America suggested a failure to apply widely held principles of fairness, careful management of resources, and shared responsibility.
The message clearly emerged that Americans want a health care system that is easy to navigate. They want to have stable coverage when circumstances change, such as when they graduate from college, change jobs, get married, or move to a different state. People want decisions about what is and what is not covered to be made in a participatory process that is transparent and accountable. These decisions would draw on best practices and be responsive to innovation in the marketplace, resulting in a clearly defined set of benefits and services for all Americans.
An important step in realizing this vision is establishing an ongoing mechanism for identifying and updating core benefits and services that would ensure access to appropriate health care for all Americans. This “core,” described in Recommendation 4, does not limit Americans to these benefits and services alone. However, it will describe a set of basic benefits that everyone should have. Most importantly, this mechanism would employ the best available evidence and promote the use of efficient, high-quality care rather than create barriers to it.
Setting a Timeline for Realizing Change
The overwhelming majority of Americans that the Working Group heard from want health care system change to begin now. Consistent with timeframes associated with other major health system reforms, the Working Group is proposing immediate action to establish the policy that all Americans have affordable health care, with a suggested target of 2012 for both implementing core benefits and services and making substantial progress in implementing the improvements that are needed to support it.
2: Guarantee Financial Protection Against Very High Health Care Costs
No one in America should be impoverished by health care costs. A national public or private program must be established to ensure:
-
Participation by all Americans
-
Protection against very high out-of-pocket medical costs for everyone
-
Financial assistance to pay for this coverage to families and individuals based on ability to pay
Context
Devastating injuries and serious illness can cost families and individuals hundreds of thousands or even millions of dollars in health care expenses. As one participant said, “homes and savings can be lost in the blink of an eye.” Out-of-pocket costs of treating an injury or illness can bankrupt not only those with little or no health insurance and modest incomes, but also many insured or wealthy families.
Many Americans already have coverage that protects them against these high costs. However, protecting all Americans against impoverishment from high health care costs is not just a simple matter of providing some form of standard coverage, because catastrophic costs are experienced relative to income and wealth.
Coverage that protects against high out-of-pocket medical costs can be designed in many ways. A number of states have designed re-insurance programs that cover the highest health care costs in the small group or individual insurance markets. Others have set up high-risk pools designed to provide coverage for people who cannot get insurance in the private market. These programs are intended to help open up private insurance markets to more people by limiting the risk that insurers face if people incur very high health care costs. Policy experts and professional organizations have proposed different types of federal programs to provide re-insurance or to protect individuals from very high out-of-pocket costs.
Stabilizing Employer-Based, Individual & Small Group Markets
Currently, many employers facing high and rising premiums are reducing their level of support for health insurance coverage to their employees. This in turn exposes more Americans to the potentially devastating financial impact of getting sick or injured. The expectation is that a policy requiring all Americans to be covered for high out-of-pocket costs would help to both stabilize existing employer-based health insurance markets and expand the private individual and small group health insurance markets. This would result in the ability to offer protection to Americans who are currently uninsured or underinsured. High-cost coverage protection would also result in lower premiums for “front end” individual, small-group, and large-group health insurance products.
If new requirements for insurance coverage are put into place, whether in a private, public, or private/public blended program, incentives to employers and individuals would change. Some employers may reduce the coverage they offer because their employees would be able to obtain this new high-cost protection coverage on their own. However, many employers who were intending to drop or reduce health insurance coverage as a fringe benefit would now participate in the purchase of high-cost protection coverage for their employees. This would result in an expansion in coverage over what would occur under current market conditions.
Relief for Public Programs
In addition to helping stabilize private health insurance markets, a federal program providing high-cost coverage could shift some burdens among federal and state programs. For example, although the federal government would have to spend more to subsidize the costs of the new coverage, it could eliminate some payments it now makes for unpaid health care bills. High-cost coverage could also provide significant relief to some public programs, including Medicaid, which in turn would give states the opportunity to redirect funds to expand coverage for low-income individuals or families or others who are uninsured or underinsured.
Ensuring Everyone Can Get and Keep Coverage
Although there are important differences in the ways that approaches to catastrophic coverage could work in a national program, any solution will have to address the basic issue of making sure everyone is able to get and keep coverage, regardless of health care status, need for services or ability to pay. Building a system that protects all Americans from very high medical costs will offer immediate help to people at serious risk. In addition, it will offer lessons on how to structure broader coverage of core benefits and services.
Features of Universal Protection:
|
After listening to and analyzing the needs and ideas of the American people and discussing the topic with experts, the Working Group developed two possible frameworks that would meet the requirements of universal protection and guard against very high health care costs: The Market–Based and the Social Insurance models.
The Market-Based Model
The basics of the market-based model are as follows:
-
All Americans would have to obtain coverage against high out-of-pocket costs.
-
Individuals would be offered a choice of standardized high-cost insurance products, whose details would be easy to understand and easy to compare.
-
The products would offer protection at different levels of out-of-pocket costs to individuals.
-
Individuals would be free to purchase the policy that best suits their needs. Since individuals with the lowest incomes also face impoverishment with all but the most expensive plans, premium subsidies would be provided based on ability to pay, and would diminish with increasing income levels.
-
Employers would retain a role in paying for or providing health plans.
| The Market-Based Model: An Example For illustrative purposes only, consider three policies covering the same set of services:
|
The Social Insurance Model
A second approach is based on a social insurance model:
-
All Americans would be required to participate in a federal government program protecting against very high out-of-pocket costs.
-
The program, like Medicare, would be administered by the federal government through private-sector contractors.
-
The program would be funded through a combination of premiums and earmarked federal revenues. Premiums would be structured to be fair and affordable, based on a sliding scale or surcharges related to income.
-
Federal subsidies, based on ability to pay, would be provided to pay premiums.
| The Social Insurance Model: An Example In an illustration of this coverage approach, protection would be provided against out-of-pocket costs for covered services that exceed some percentage of income—such as 20 percent of taxable income above the federal poverty level—or that exceed a fixed dollar amount of individual liability—such as $30,000—whichever is lower. |
3: Foster Innovative Integrated Community Health Networks
The federal government will provide leadership and financing for a national initiative to develop and expand integrated public/private community networks of health care providers. This recommendation should be accomplished through the following actions:
-
Focus first on people and localities where improved access to high quality care is most needed. These networks would offer local residents – including, but not limited to, low-income and uninsured individuals and people living in rural and underserved areas – a source of coordinated health care.
-
Identify governmental agencies at the national, state and local levels to coordinate private and public funding sources currently dedicated to helping provide care to the underserved by supplying the necessary information and leadership.
-
Establish a public/private group or not-for-profit entity at the national level responsible for advising the federal government on the community health care network’s performance, funding streams, best practices and research.
-
Expand and modify the Federally Qualified Health Center concept to accommodate other community-based health centers and practices serving vulnerable populations with special emphasis on families and prevention.
Context
At community meetings and through online discussions, the Citizens’ Health Care Working Group heard stories about the difficulties many people face obtaining health care. While anyone can experience these problems, they are especially severe for certain populations, particularly those with lower incomes, who lack insurance, or who live in underserved areas.
“Fix the delivery system first,” was the closing comment at one community meeting and a sentiment expressed throughout the public engagement process and by many experts. Among the many delivery system problems cited were: a lack of primary-care providers, the inability to access specialty care, and difficulties in navigating a complicated system, especially for those with chronic conditions.
Participants emphasized the importance of having access to health care in their local communities and the need to keep systems simple and easy to navigate. Citizens in multiple locations spoke highly of the continuity of care and easy access to needed services they receive from some of the large, integrated delivery systems and health plans.
Across the board, citizens expressed strong support for neighborhood health clinics. When asked about ways to help ensure access to affordable health care services, participants consistently ranked expanding community health clinics as the second or third choice. Online, 74 percent of respondents either agreed or strongly agreed with such expansion.
The Current Picture
The Working Group has been impressed by the creativity and energy some localities have brought to improving their health care delivery systems. Many of these localities have successfully coordinated public and private funding sources to achieve seamless local systems of care that address health care needs throughout the lifespan. Examples of such local initiatives are described in The Health Report to the American People.
However, despite these positive examples, more needs to be done to fill gaps in both financial support to and services provided by local health care providers and organizations. Efforts to do so will allow these networks to function as truly integrated community systems.
At present, local providers negotiate a host of diverse funding programs targeted at different subpopulations, from a variety of state and local government agencies as well as national, regional, and local philanthropic organizations, foundations and other private organizations. Community systems also receive reimbursement for services from public and private insurers and direct payments from patients.
The result is a mixture of revenue streams, with each source beginning or ending at different times. From this ever-changing pool of funding, local systems must design a set of short-term programs providing services some of the time to some of the people. Inconsistencies in services provided and population served contribute to confusion, frustration and missed opportunities.
In order to meet their full potential to serve those most in need, these systems must be able to devote more of their energies and talents to the provision and management of care. As one participant remarked, “by assisting the development of community-based health care centers, we begin offering services at more convenient times for the ever busy American public and take pressure off the emergency room systems.”
Developing Innovative Integrated Community Networks
At meetings, participants described a vision of an integrated community network. It would be a system where health care providers at the local level work together to ensure:
-
Everyone has a “medical home” and access to primary, mental, and dental health care
-
Wellness and prevention are emphasized at the community level
-
Referrals to medical specialists, hospitals, and other providers, when necessary, are made easily and follow-ups are made consistently
-
Medical records are available to providers within the network when needed and in full compliance with privacy laws
-
Evidence-based care is delivered effectively and efficiently, making use of certified nurse practitioners, licensed visiting and practical nurses, medical assistants and other physician extenders
-
Patients do not encounter bureaucratic barriers in seeking and receiving appropriate care
Primary care, as the entry point for the health care system, is the foundation of an integrated network. But the networks also could play an important role in coordinating care for people with acute and chronic health conditions, as well as offer mental health and dental health care. In addition, they should further best practices in health promotion and prevention, including services such as health education, nutrition counseling, and wellness checks to the healthy members of their communities. In essence, community networks can provide the tools needed to help everyone in the community be good stewards of their health and their health care.
The Working Group has concluded that a community-centered approach will not only be good for the health of individuals but also will improve the community’s general well-being. These networks should be open to all who wish to participate—with special efforts being made to find, connect with, and offer needed support to those who are most in need of help.
Expanding What Works: Technology, Innovation, Federal Support
Better communication across providers of care is essential to sharing resources and reducing duplication of effort. This can be facilitated through the use of new technologies, in particular, electronic health records and telemedicine. Implementing these technologies at the community level has the potential to benefit community providers and their patients by improving the continuity of care, reducing duplication and medical errors, and providing increased access to specialty care for individuals in urban, as well as remote and isolated areas.
Encouraging innovation at the community level through new or expanded public/private partnerships is central to improving community health networks. Public support, both structural and financial, from all levels of government, will give any community the tools it needs to better coordinate and manage the health resources already at its disposal.
In addition, the Working Group recommends that some of the eligibility requirements for Federally Qualified Health Centers be modified for community-based health care providers offering comparable services to similar populations. With certain exceptions, benefits at the federal government level, such as grant funding, cost-based reimbursement, access to reduced-price prescription drugs, and malpractice liability coverage under the Federal Tort Claims Act, are limited to Federally Qualified Health Centers. Expanding these benefits would serve as an incentive for a community-based organization to participate in an integrated network.
Americans in the community meetings expressed approval of and appreciation for responsive, accessible local health care. Fostering integrated community health networks through these changes will build on current successes and strengthen the safety net for those who need it most while expanding innovative health care to more Americans.
4: Define Core Benefits and Services for All Americans
Establish a nonpartisan public/private group to define America’s core benefits and services and to update it on an ongoing basis
-
Members will be appointed through a process defined in law that includes citizens who represent a broad spectrum of the population, including, but not limited to, patients, providers and payers.
-
The group will be staffed by experts.
-
Identification of core benefits and services will be made through an independent, fair, transparent, and scientific process.
Within economic constraints and guided by evidence-based science and expert consensus regarding the medical effectiveness of treatments, the group will define the core benefits and services based on the following principles:
-
Core health services will cover the continuum of care throughout the individual’s lifespan.
-
Health care encompasses wellness, preventive services, primary care, acute care, prescription drugs, patient education, and the treatment and management of health problems provided across a full range of inpatient and outpatient settings.
-
Health is defined to include physical, mental, and dental health.
-
Over time, this entity would appropriately take into consideration advances in clinical science
Context
The conversations in each and every community meeting demonstrated how difficult the task of defining basic health care coverage will be for policymakers. In almost every instance, groups of citizens could not agree on much except including everything in a basic benefit plan. Discussion groups had difficulty reaching consensus about what types of services would be optional, reflecting how differently people value services and types of care.
Participants made it clear that they trusted their fellow citizens and medical providers and, to a lesser degree, governments to make the tough choices in the absence of unlimited resources. They also expressed a clear interest in using sound information on cost-effectiveness as criteria for making smart choices.
As was the case in many deliberations, the public was aware of the political challenges involved in making such decisions. They highlighted the virtues of independent commissions along the lines of the “Base Closing Commission” in helping policymakers with such choices. Several times it was suggested that “some new entity or process needs to be created that includes all the relevant stakeholders, the foremost of which would be the consumer.” Consequently, the Working Group recommends the creation of a structured process and guidelines for how decisions are made when determining what should be included in a core benefit package.
Determining Core Benefits and Services
To define a set of benefits and services that works for all Americans, the best methods must be applied in a transparent process. Consumer participation is critical to ensuring public trust in the process and that personal values and preferences are taken into consideration in coverage decisions. The group making decisions would be established as a public/private entity to insulate it from both political and financial influence. The group would be an ongoing entity with stable funding, to guarantee its independence and to ensure that coverage continues to be responsive to evolving medical knowledge and practice.
The work of this entity can simultaneously help to make all health care more effective and efficient, while aiding to control health care costs overall. This recommendation works in conjunction with the recommendation on efficiency, effectiveness, and quality of care because up-to-date evidence on what works best in health care will be the basis for decisions about the benefits and services included in the core set.
Defining benefits and services can be accomplished through a structured, participatory process. Decisions would be based on assessments of how important it is to ensure that treatment is covered while taking into consideration the effect on individuals’ health, public health, and the effectiveness of treatment options. The process would include full participation of consumers, health care providers, and relevant experts.
This process of identifying core benefits should also reinforce the principle of comprehensive health care coverage through a system of shared responsibility. Evidence used to make decisions about coverage can contribute to improvements in the overall efficiency of health care delivery and help patients and providers make informed decisions. Sound evidence could also provide a way to link cost sharing to more efficient health care.
Evidence-Based Practices as a Foundation
The core benefits will be developed using the growing body of evidence on the effectiveness of medical therapies, procedures, and devices. This information is based on specific levels of evidence, such as clinical trials, effectiveness studies, comprehensive reviews of published analyses, and expert consensus. It is being gathered through ongoing processes organized by professional organizations and providers, state-led efforts to inform coverage policy for Medicaid and the State Children’s Health Insurance Program, federal activities such as the U.S. Preventive Services Task Force and the Evidence-Based Practice Centers and supported by the Agency for Healthcare Research and Quality, and international collaborations focused on assessing the effectiveness of clinical care.
The group would draw upon these multiple sources of expertise to establish a clear set of rules for assessing the evidence that will, in turn, be used to determine benefits and services included in the core set and to update it when appropriate.
A Fair, Evidence-Based System to Determine Benefits
A look at the graphic representation below reveals how this process of defining benefits could work:
-
The vertical arrow represents a structured process that identifies, then prioritizes the medical conditions and the treatments and services that need to be covered.
-
The horizontal arrow represents the efficiency of specific treatments or services, based on credible evidence that takes into account cost-effectiveness.
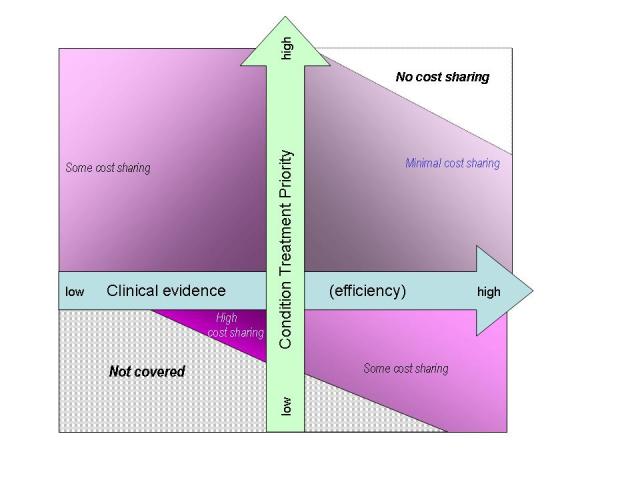
Benefit design can promote more efficient health care
By way of illustration, if there are two equally effective ways to treat a particular medical condition, but one costs twice as much as the other, the less expensive treatment would have a higher efficiency rating. Health services and treatments that are deemed essential and cost-effective could be offered with little or no cost-sharing. Certain kinds of preventive care, such as childhood vaccinations, would be prime examples. Treatments that have not been proven to be medically effective would not be covered at all, to discourage their use. People who choose to obtain treatments or services proven to be not as cost-effective as covered alternatives would pay more of the costs for that care.
Aligning the Core Benefits with Current Coverage
Most people currently get their health coverage through employer sponsored insurance, while more than a quarter of all Americans receive health care coverage from a public program. Establishing a core set of benefits and services for all Americans means reassessing the benefits currently provided in both public and private programs. Coverage and benefits vary across types of employment or industry, local insurance markets, and public programs reflecting specific requirements set out in law, as well as policies driven by budgetary constraints and other factors.
For many people covered by public programs, the services and benefits being provided represent specific forms of commitment that society has made to tens of millions of women and children living in poverty, people with disabilities, people who are elderly, veterans and military families, Native Americans, and others. Benefits often cover a broad spectrum of health care reflecting the needs of these specific populations and can include prescription drug coverage, mental health assistance, personal services, dental care, and vision and hearing services.
The core set that results from this process may look different from many public and private systems. It would likely be broader in some respects than the current Medicare benefits package. For example, Medicare’s mental health coverage is very limited, and hearing and vision services are generally not covered. If broader coverage contributes to more effective treatment and management of illness, changes to Medicare’s benefit package would be appropriate.
The Working Group understands that some services may not be included. Some benefits and support services now covered by Medicaid can help people with disabilities and serious chronic illnesses live as productively as possible in their homes and communities. Since specifically targeted programs, including those that are part of state Medicaid systems, can provide some of these services more effectively, and some of these services include nonmedical support, they may not be covered as core benefits. Examples include personal assistance and respite services, medical supplies and assistive devices, home and vehicle modifications and transportation services. As discussed in Recommendation 6, on end-of-life care, these services, along with the full range of long-term care services that will become increasingly important as society ages, need to be integrated more effectively in a health care system that works for everyone.
Similarly, the core benefits may be more generous than benefit packages of some employer based plans and less generous than others. However, establishing a core set of benefits and services, reflecting sound medical evidence, as a standard against which any coverage plan can be evaluated will go a long way toward creating health care that works for all Americans.
5: Promote Efforts to Improve Quality of Care and Efficiency
The federal government will expand and accelerate its use of public programs for advancing strategies that improve quality and efficiency across the health care system.
Using federally funded health care programs, the federal government will promote:
-
Integrated health care systems built around evidence-based best practices
-
Health information technologies and electronic health record systems
-
Elimination of fraud and waste in administration and clinical practices
-
Widespread availability of consumer-friendly information about health care services, including transparency on prices, cost-sharing, quality, efficiency, and benefits
-
Increased focus on health education, disease prevention and health promotion, patient-provider communication, and patient-centered care
-
Biomedical research aimed at improved quality and efficiency
Context
Throughout the public discourse, major concerns were voiced repeatedly: How can America do a better job with the two trillion dollars a year spent on health? What can be done to achieve greater efficiency and improve quality?
Part of the public’s interest stemmed from concerns about the cost of health care and what many perceived as waste and inefficiency in the current system. Many spoke out about administrative costs and profits, often pointing in particular to the high costs of prescription drugs and a frustration with for-profit health insurance. A common theme was “Who, or what, is the current system designed to serve—the patients or the health care industry?” As one participant remarked, “it is often more stressful to deal with the insurance company than the disease.” Review of the evidence suggests that what is driving health care costs may not be as simple or easy to fix as many people have come to believe. But the problems are very real and there is clear support for initiatives to tackle the issues surrounding efficiency and quality of health care in America.
The public saw a connection between quality and cost. For example, many agreed that greater investment in health information technology and moving to an integrated system of electronic health records could improve administration and treatment while reducing medical errors. More than two-thirds of respondents to the Internet poll supported more investment by doctors, hospitals, and other providers in health information technology as a means to improve quality and increase administrative efficiency. Furthermore, many participants in the community meetings discussed the desirability of using medical evidence to decide which services are covered and provided. Similar results have been found in national polls.
Individuals have the ability and the desire to be informed health care consumers and a positive influence in efficient treatment decisions. On the one hand, people expressed a need to have more information about how to use health care better and more effectively. This is a sentiment found in national polls which show that many Americans believe they do not have enough information about hospitals and other health care facilities to make educated health care choices. One participant suggested that Americans “would be willing to pay for some of the cost of their care if they could understand up front the risks, costs, and benefits of different treatments for their medical maladies.” On the other hand, concerns were voiced about a family’s difficulty making informed medical decisions in times of crisis.
The Cost of Poor Quality Care
Above all, it is clear that the economic cost of poor quality health care and medical errors is high. These costs are in addition to the pain and suffering – and in some cases, the loss of life – resulting from overuse, underuse, and misuse of medical services.
Waste in the health care system can take many different forms. Examples include: unnecessary care induced by excess capacity (e.g., using hospitals, diagnostic equipment, physicians simply because they are available), a failure to avoid preventable complications (such as reactions to medications and some hospital-acquired infections) and the associated costs of additional care delivery, and inefficiencies, especially those resulting from a fragmented delivery system. These examples do not include costs associated with the underuse of proven diagnostic and preventive protocols that can forestall treatment of preventable medical conditions. Additionally, one must take into account the indirect costs to individuals and employers of lost productivity and earnings.
Experts who testified at Working Group hearings estimated that the total costs of health care for the nation could fall by 32 percent, and survival rates increase by 2 percent, if all communities were to utilize medical specialists, hospital beds, and ICU beds at the same rate currently used by some leading integrated delivery systems in the United States. Additional cost savings may reasonably come from chronic disease management and reductions in care-associated injuries. A forthcoming report supported by the Agency for Healthcare Research and Quality of front-line inefficiency, as health care providers struggle with a massively complex, poorly coordinated, health care enterprise, categorized 35 percent of all efforts as waste. Taking the testimony and study together indicates that a significant portion of all health care expenditures produce no added health value. Fraud and abuse, while relatively small compared to the health care system’s problems discussed above, still correspond to significant additional economic losses and represent opportunities for improved care at a lower cost.
Concentrated efforts in some integrated health care systems have demonstrated care can be improved and waste eliminated. Continuous improvement methods have reduced costs by optimally managing chronic conditions, reducing preventable care-associated patient injuries, and designing coordinated systems of care delivery that reduce hassle and rework.
However, continuous improvement efforts rest on fundamental change in underlying medical practice and professional culture – a difficult, long-term, proposition. Widespread improvement will require a much better understanding of how to “do it better” (investment in health care delivery research), restructured training programs, significant organizational restructuring, and investment in aligned health information technologies and systems. To date, most early successes have come in integrated delivery systems, which have the concentrated resources and organizational structures to address these needs.
The ramifications are clear—improvements in health care outcomes that produce significant cost reductions are achievable, but over the long run. Success will require fully integrated systems of care as well as committed management.
Building on Existing Models for Change
Important, innovative work in quality and efficiency improvement is under way in a number of local and regional private systems around the country as well as in government programs. New initiatives being tested—often with the private sector and federal government working together—allow doctors, clinics, and hospitals to share medical information safely and efficiently.
Health care providers, employers who purchase health care, and public programs are all working together to reduce preventable medical mistakes. These groups are testing ways to measure performance of physicians, hospitals, and other health care providers by using data available to the public. They are trying out ways to use information on provider performance to reward high-quality providers and to reward consumers for using more efficient, higher quality providers. Some employers are introducing innovative practices to enhance employee health that may also reduce costs. For example, some support wellness centers and physical fitness facilities. Others are using financial incentives to encourage employees to stop smoking or lose weight.
The federal government has also been active in this field. The Veterans Health Administration has been developing performance measures as a basis for improving care and efficiency in clinical settings. The Centers for Medicare and Medicaid Services participates with several private and public groups to promote quality care and measurement and has introduced a number of its own initiatives in the areas of nursing homes, home health, hospitals, physicians, and end-stage renal disease care. Development of quality measures, especially when these can be related to evidence-based medical practice, is a key component of any strategy to improve quality and reduce unwarranted practice variation. In August of 2006, the Secretary of Health and Human Services announced a new initiative to facilitate and promote wider and more effective use of quality measurement tools and health information technology.
Efforts in both the public and private sectors can also help to ensure the benefits of ground breaking biomedical research that hold great potential for prevention and treatment of disease are, in fact, used effectively.
Federal Government Leverage
In the Working Group’s Internet poll, participants overwhelmingly supported the view that both the public and private sector play a role in improving efficiency.
With this in mind, it is crucial to consider the implications of the federal government’s role as a dominant purchaser of health care. It also plays a significant role in the research and evaluation of the delivery of health care services. Therefore, it is well positioned to provide leadership in this field.
A variety of federal programs could be used for development, demonstration, and dissemination of reform efforts. These programs run the full range of design possibilities, making them particularly useful for “beta testing” of new ideas.
Health care researchers and practitioners are well aware of the practical difficulties of replicating these improvements on a wide scale. To do so will take concerted public/private effort and strong leadership. The federal government should work with private sector organizations to ensure that these programs are evaluated fully and fairly.
As noted earlier, there are federal agencies like the Agency for Healthcare Research and Quality and the Centers for Medicare and Medicaid Services (within the Department of Health and Human Services) that already support evaluations. However, in order to fully realize this advantage, they may need to broaden the scope of their demonstrations and experiments and, perhaps, seek expanded authority to do so. If successful quality improvement efforts can be adopted by significant numbers of providers, the cost savings and improved health outcomes might spur a truly fundamental reform of the nation’s health care system.
6: Fundamentally Restructure the Way End-of-Life Services are Financed and Provided
End-of-life care should be fundamentally restructured so that people of all ages have increased access to these services in the environment they choose.
-
Public and private payers should integrate evidence-based science, expert consensus, linguistically appropriate and culturally sensitive end-of-life care models so that health services and community-based care can better handle the clinical realities and actual needs of patients of any age and their families.
-
Public and private programs should develop and support training for health care professionals that emphasizes proactive, individualized care planning and clear communication between providers, patients and their families.
-
At the community level, funding should be made available for support services, including nonmedical services, to assist individuals and families in accessing the kind of care they want for the last days of their lives.
Context
End-of-life care surfaced as an issue at virtually every community meeting held by the Working Group. Americans clearly agree that alternatives to medical and surgical interventions of questionable value for people with advanced incurable illnesses and for those nearing the end of life should be encouraged. Many argue that current end-of-life care is expensive, that it often does not improve the patient’s quality of life, that it is too often based in hospitals or nursing homes and that it may not be consistent with the wishes of the patient or family.
In place of those interventions, the people we heard from expressed preferences for providing at-home and comfort care. There was a desire for individuals nearing the end of life and their families to receive support from the health care system in understanding their options, making their choices about care delivery known, and having those choices honored. Greater emphasis on providing palliative care met with strong support in the Internet poll and community meetings, with 61 percent and 63 percent, respectively, agreeing or strongly agreeing.
End-of-life care is not restricted to the elderly. At some community meetings, participants expressed concerns about the difficult issues surrounding the care of other populations with terminal medical conditions, including very low-birth-weight babies.
Discussions at all community meetings underscored the importance of this issue to Americans. A community meeting was held in New Hampshire that focused specifically on end-of-life issues. Values expressed by meeting participants included honoring personal choices, providing adequate pain relief, and ensuring that health professionals treat persons nearing the end of life with dignity and respect. Importantly, it was noted that payment incentives for end-of-life care are currently misaligned with these values. The current system encourages heroic interventions in hospitals and care in nursing homes in lieu of low technology care, support, and time spent with health care providers.
Also playing an important role in end-of-life care are nonmedical services, such as transportation, personal care, and assistance with meal preparation. New models of care delivery must do better at taking into account language barriers and cultural differences. However, it is most essential that care is focused on maintaining the dignity of patients in their last days.
Cost, Quality and Efficiency
A major fear for many people as they approach death is the financial burden their care may place on their families. It has been estimated that expenses in the last year of life constitute 22 percent of all medical expenditures. New models of care delivery should do a better job of knitting together community-based services—often nonmedical—to meet the needs of people nearing the end of life and their families.
A new model of care becomes even more critical as people live longer with chronic conditions. A stronger focus on knowing both what works and when medical intervention serves no good purpose, coupled with more consumer-friendly information and better provider-patient communication, will help seriously ill people and their families make informed choices about care. More information on quality and efficiency will also begin to address the current substantial regional variations in intensity and cost of health services used by the elderly, aligning these variations to outcomes.
When developing a new model of care, there is much to learn from leaders in the field of palliative care such as the Hertzberg Palliative Care Institute at the Mount Sinai School of Medicine in New York City. Also, the demonstration projects funded by the Robert Wood Johnson Foundation from 1998 through 2004 in its “Promoting Excellence in End-of-Life Care” initiative offer examples of new care delivery models that emphasize coordination and continuity of care.
Helping Americans have the “good death” they desire will require change. At the policy level, new care models must address the extended periods of fragility many Americans experience. Payment policies and professional medical training programs must be adjusted accordingly. For example, Medicare reimbursement for hospice services needs to better account for the most common patterns of death and dying while accommodating the differing trajectories of common causes of death. Payment for providers needs to be less procedure-driven and take into account essential time-intensive services such as provider-patient counseling and guidance. End-of-life care must become a central training component for all health professionals who have direct patient contact.
Serious illness and death can occur at any age. As new models for care delivery and patient and family support mechanisms develop, the special problems faced by terminally ill newborns or children and their families must be considered as well.
Areas of Need Extend Beyond the Health Care System
A comprehensive system of care for the dying extends beyond the health care system. Here are a few areas that must be considered when restructuring end-of-life care:
-
Professional and family caregivers: More attention needs to be given to professional caregivers as well as to family members who become caregivers. Direct-care workers usually receive low wages and few benefits. They often work part-time and are themselves uninsured. As the number of elderly Americans increases and more caregiver services are required, the system will need to offer better pay, improvements in training, and opportunities for professional growth in order to meet the increasing demand.
-
Objective, useful information on needs: Policy development is currently hampered by a lack of useful information about patients, their needs, and their use of services. The development and use of standardized instruments for collecting demographic, epidemiological, and clinical information, careful evaluation of emerging care models, and the dissemination of best practices are all needed to improve care for the dying.
The concerned and thoughtful attention to end-of-life issues that emerged through the public dialogue made clear to the Working Group that change is needed. The passion expressed by participants emphasized the importance of such change. The Working Group acknowledges that end-of-life issues are often difficult, painful, and complicated and thus not conducive to quick or easy fixes. One person commenting on the Working Group’s web site said, “When one is reaching the end of life, it’s hard and unimaginable to think that you and your loved ones are not getting the proper support.” This recommendation seeks to better define, communicate, and make available at individual, family, community, and societal levels the support needed and wanted in one’s last days.
PAYING FOR HEALTH CARE FOR ALL AMERICANS
No plan to address the serious shortcomings in today’s health care system would be complete without considering how to pay for it. In doing so, the Working Group members considered the discussions at community meetings, citizens’ comments received in its web-based polls, and public opinion expressed in national polls. Members also discussed a number of proposals put forth by government agencies, think tanks, and scholars.
The Working Group arrived at three guiding principles to financing new initiatives:
-
The financing methods should be fair. Fairness is evaluated using three factors. First, financing methods should not have the effect of creating a disproportionate increase in the financial burden on the sick; second, responsibility for financing of health care should be related to a household’s ability to pay; and third all segments of society should contribute to paying for health care.
-
The financing methods should increase incentives for economic efficiency in the health sector and the larger economy.
-
The methods should be able to realize sufficient funds to pay for the recommended actions.
As noted above, everyone – government, families, and businesses – must be involved in improving health care. The Working Group heard over and over again that everyone has a stake and everyone must contribute.
Overview of Approach
The Working Group believes that a number of the recommendations made in this report force a difficult choice of finding sources to pay for these actions or contributing to sizable budget deficits.
The Working Group believes that some of its proposed actions would result in opportunities to reallocate existing funds spent by state and federal governments. These would include payments by Medicaid under disproportionate share (DSH) provisions, high-cost risk pools, and uncompensated care payment programs.
Some of the actions proposed in this report may also yield savings to the health care system in the long term (as noted in the discussion on quality and efficiency). Since these recommendations call for immediate action to develop protection against high health care costs and investment in further development of integrated community health networks, some funds will be required right away. Based on the evidence and conversations with experts, the Working Group has concluded it is unlikely that health system improvements will yield sufficient savings over the next few years to pay for some of the reforms recommended in this document.
In addition to reallocating existing funds and harnessing savings, a third source of financing would stem from making changes in existing government subsidy programs that are at once inefficient and unfair. Based on recent reviews of federal subsidy programs by the Congressional Budget Office (including the Annual CBO Budget Options), the President’s Commission on Tax Reform and independent scholars from across the political spectrum, the Working Group believes that significant funds would be available by altering such public subsidy programs in a way that improves both economic efficiency and fairness.
Finally, if these sources were not sufficient to address the funding requirements of the six recommendations presented, new revenues would have to be considered.
The Working Group strongly believes that in order to gain the confidence of the American public it is critical that funds obtained from reallocations, savings, changes in subsidy arrangements, or new revenues be specifically dedicated to health care coverage.
Citizen Input on Financing Issues
Based on a review of national polls, the Working Group’s own Internet polls and discussions at community meetings, it is clear that a very large segment of the American people believe there are sufficient funds associated with American health care to pay for health care that works for all Americans. As a result, there is a strong sense in the public that reallocation of existing public funds, changes in subsidy programs, and increased efficiency should take priority in funding the recommended actions.
Yet when posed questions about the possible need for new revenues, we found, across the board, that majorities of the population were willing to pay more to ensure that all Americans are covered. This has also been found consistently in national polls. The specific option raised most often in meetings and comments was some form of progressive, or "sliding scale" income or payroll tax (like the Medicare payroll tax) specifically dedicated to supporting health care for all. Some who supported this approach to financing indicated that they personally could not afford to pay any more; health care costs have strained their budgets to the limit. A smaller group of respondents expressed strong opposition to any form of taxation at all.
We also heard other specific proposals for raising revenues to support health care for all Americans. Some examples follow.
“Some sort of a general consumption tax (sales tax) adjusted for the product based on factors such as its healthfulness and use to low vs. high income consumers (e.g., 1% on grocery products, 10% on fast food, 2% on a used car, 5% on a new car, 1% on a canoe, 8% on a power boat, etc.) could be the fairest.”
“I believe this can be financed with greater (and enforced) corporate income taxes, graduated enrollee contributions, and the like. Fairness demands that the revenue not come from sales tax or any tax that has the greatest impact on the Americans who have the least income.”
“Short-term security for Americans at risk should be from the federal and local tax bases. I say yes to a “sin” tax.”
“It seems to me that fairest, least complicated way to fund an affordable, accessible health care system for everyone is through an income tax deduction or a value-added tax. How about a 5% tax on every soft drink sold in America?”
The Cost of Inaction
If the United States Congress decides that fundamental change in health care is either too disruptive to the economy, too complex, or too controversial and defers further action at this time, the Working Group fears that the cost of this inaction to American families goes beyond dollars and cents.
The problem of medical providers charging the insured more to cover costs of the uninsured will become even more prevalent. Public budgets will continue to feel the pressure of both the growing numbers of uninsured people and of the aging population, as long-term care costs consume an even greater share of Medicaid funds. Additionally, uncompensated care costs—now estimated to be more than $40 billion annually—will continue to rise, placing huge burdens on hospital providers and even forcing many safety net providers to close.
Furthermore, health care premiums will continue to rise. These increases will make it more difficult for many businesses to continue coverage for their workers and retirees; they will continue paring down coverage and shifting costs to employees. Individuals and families will find it more difficult to purchase coverage from their employers or the individual market and may not be eligible for public programs. States will continue to explore ways to provide coverage to their residents, but finding the revenue to pay for these programs could threaten budgets or lead states to raise revenues in ways that drive out businesses. The uninsured will continue to receive less care and less timely care, to sustain more financial risk and to live, on average, shorter lives. The ramifications of the changes above will reach to every facet of American society, fundamentally altering the economy from what it is today.
A do-nothing response today will merely delay this impending crisis for others to tackle at a later date, at which time the size of the problem—the cost of inaction—will be much larger.
The Citizens’ Health Care Working Group urges timely action on these recommendations for making health care work for all Americans.
COMMENTS
TRANSFORMED U.S. HEALTH CARE SYSTEM
Alternative Perspectives to the Working Group Majority’s Recommendations
Author: Randy Johnson, September 2006
Summary
The Citizens’ Health Care Working Group (CHCWG) was appointed by the U.S. Comptroller General in accordance with provisions included in the Medicare Modernization Act, and charged with submitting recommendations to the President and Congress that would result in “Health Care that Works for all Americans.”
“The Health Report to the American People,” released by the Working Group in October 2005, indicates the average annual health care cost per person in 2004 was $6,300 and projected to be $11,000 by 2014. Despite the increasing cost, patients receive only 55 percent of the care recommended by experts, and, according to the Institute of Medicine, there are as many as 98,000 deaths annually due to medical errors in hospitals. The U.S. Census Bureau has reported that 84 percent of us in the U.S., more than 247 million, have health insurance (approximately 175 million in employer-based programs, 40 million in Medicare, 38 million in Medicaid, 27 million in direct purchase programs, and 11 million in military programs with some having coverage under more than one type of program). Yet, approximately 47 million people (about 16 percent) in the United States do not have health insurance. So, reducing costs, improving quality, reducing waste and errors, and ensuring coverage are the critical elements required to fix our health care system.
This paper provides alternative recommendations to those of the Working Group majority due, in part, to concerns related to the “dialogue with American citizens” (see “Process” section below).
1. The following recommendations are based on expert testimony from the hearings, input from the community meetings, recent trends by employees who are covered by health plans today as well as my own experience in developing and implementing health care initiatives for 30-plus years.
2. Recognizing the current U.S. entitlement programs’ obligations, the focus of “shared responsibility” rests more on individuals and less on the government.
3. The following depend more on private initiatives and less on government solutions.
Alternative Recommendations to Transform the U.S. Health Care System
The following illustrative recommendations are alternatives to those of the Working Group majority. They build on the strengths of the current U.S. health care system and are founded on two premises: 1) the U.S. has dedicated, expert, resourceful medical professionals, and 2) market-based systems have historically served the U.S. well. These recommendations are designed to improve quality and efficiency, and make coverage available to all Americans.
I. Fundamentally, the U.S. Health Care System Must Be Transformed with Dramatically Improved Quality and Efficiency. Without improvements in these areas (expected by health care leaders from both the private and public sectors) from initiatives already being implemented, more citizens will likely move to the ranks of the uninsured, patients will continue to receive care that doesn’t meet quality standards and lives will unnecessarily be lost.
A. By 2007, provide legislation and regulations to fund the National Quality Forum’s adoption of uniform nationwide measures of quality, and provide for the following in Medicare, Medicaid, FEHP, TRICARE and other federal and state health care programs:
1. Implement measurement, transparency and disclosure of outcomes.
2. Increase assistance for patients and other consumers in the following ways:
a. Give them information and tools to make informed decisions.
b. Focus on preventive care and protocols for chronic conditions.
c. Give patients strategic financial discretion (not merely cost shifting for cost-shifting purposes).
3. Pay hospitals and providers based on their performance.
The Working Group heard testimony that taking these steps could result in a 40 percent quality improvement and 30 percent gain in efficiency (reduced costs). These steps could play a major role in offsetting the costs of expanded coverage.
B. By 2007, adopt legislation and regulations that provide for funding of a private and public collaboration to adopt uniform health information standards and terminology. Also, provide funding for the implementation of health information technology, including an electronic medical record in Medicare, Medicaid, FEHP, TRICARE and all other federal health care programs where such funding results directly in quality of care improvements.
The Working Group has received input that implementation of health information technology could result in a $70 – 90 billion annual cost reduction, PLUS improve patient quality and safety. Savings can assist coverage expansion.
C. By 2008, adopt legislation and regulations to facilitate patient and family education and election of palliative care, rather than primarily curative care, in private and public health programs during late stages in life. Expected results: quality improvements in patient and family care as well as costs savings.
D. With the consideration of input from a private/federal/state panel of experts, develop alternatives that simplify the design, funding and administration of Medicare, Medicaid and SCHIP so that citizens who are covered under more than one of these programs will be able to obtain coverage and care seamlessly, and the programs will be financed with increased transparency and efficiency.
Potential results: Patient satisfaction improvement and cost reductions.
II. Retain the Strengths of the Current Employer-Based System and Expand Options so that Citizens Can Obtain Health Care Coverage when not Covered by Employer-Sponsored Plans.
A. By 2008, adopt legislation to allow access through the Medicare system for citizens age 55 and older who do not have other insurance. Use age-based rates without adjustment for pre-existing conditions.
B. By 2008, adopt legislation to allow citizens under age 55 who do not have other insurance, access to the Federal Employees’ Health Plan. Use age-based rates without adjustment for pre-existing conditions.
C. By 2008, enhance opportunities for citizens to invest funds for retiree medical coverage and purchase individual retiree medical coverage with preferential tax treatment similar to that of those covered by employer-sponsored plans.
D. By 2008, adopt legislation that allows individuals and small employers to join private health plan associations under the following provisions:
1. Enable citizens to choose coverage from insurance companies nationwide.
2. Fund government risk pools in a manner similar to stop-loss insurance.
3. Ensure that health care conditions do not result in rejection or increased premiums.
E. By 2009, require all U.S. citizens to have, at least, “basic/catastrophic health insurance coverage that includes preventive care and wellness initiatives. What is “basic/catastrophic health insurance” would be recommended by a multi-stakeholder group with representation similar to the National Quality Forum. It would be based on evidence-based design, and adopted by Congress using congressional rules that minimize the political forces that detract from best policy.
F. By 2009, increase the number of community health centers as one alternative to improve access to “basic/catastrophic coverage.”
G. By 2009, adopt legislation that allows employers to “pass the sponsorship” of health plans to “qualified sponsors” that “elect” to serve in the sponsor role. This would result in a more consolidated, efficient purchasing entity, especially for small employers, to contract with health plans or other health delivery system vendors in behalf of employees.
H. By 2009, adopt legislation which provides for a private-public collaboration, similar to the MedPAC, to recommend the government subsidy to be provided to low income individuals enabling them to obtain coverage.
I. Consider potential revenue resulting from savings due to (1) minus the cost of (2) below:
1. Establish a “cap” on the value of health care coverage that is exempted from income of employees who are covered by employer-sponsored health plans.
2. Provide similar tax treatment for individuals who purchase their own insurance coverage as provided for those who are covered by employer-sponsored plans.
J. Consider potential cost reductions resulting from changes in Medicare reforms such as:
1. Gradual deferred eligibility age.
2. Gradual replacement of the current Medicare design with “basic/catastrophic coverage” discussed above.
The Process Used to Develop Recommendations
Nationwide experts provided testimony about both U.S. health care challenges and potential solutions. Citizens attended community meetings and provided their insights and perspectives. However, it became clear that the voices not as often heard were those who actually sponsor and/or are covered by employer-sponsored health plans (e.g., administrative assistants, nonunion production workers, tellers, engineers, accountants, chemists, supervisors, and managers).
There have been additional factors in the process that, if different, may have resulted in increased credibility for the basis of the Working Group recommendations:
1. The Working Group conducted hearings that resulted in significant input to improve quality and efficiency from very prominent purchaser and union organizations. Yet, the “Health Report to the American People” essentially omitted recommendations by the business community, unions and other organizations to improve the system.
This resulted in an incomplete report. It also apparently led some organizations to conclude that since the Working Group did not consider such perspectives in the “Health Report to the American People,” it would likely omit these kinds of proposals in its final recommendations. Accordingly, some of these types of organizations concluded that their support of community meetings would not be valued.
2. The legislation called for “an informed national debate.” Yet, comments at the Community Meetings often reflected the critical need to elevate the public’s knowledge of basic facts rather than an informed discussion. Community Meeting attendees’ comments reflected misunderstandings and factual errors regarding tax treatment related to health care, insurance company profits, health plan design, current initiatives to improve the system, etc.
Health care is such a difficult subject that many may not understand the complexity and resulting implications of system design changes. Public policies based upon such incorrect assumptions or factual errors are likely to be misdirected and fail.
Thus, it is imperative for public policy to respond to many real problems in the health care system while still following the well-known medical principle, “first, do no harm.” All proposed solutions need to be very carefully considered to ensure that responding to certain points of view – however legitimate those concerns may be – does not inadvertently undermine the strengths of the current health care system.
Conclusion
“Health Care that Works for All Americans” is possible within the strengths of the current system: measurement, transparency and disclosure of health care outcomes; information, incentives and tools for consumers and purchasers to make informed decisions; payment of hospitals and clinicians based on their performance; implementation of health information technology; and new coverage option.
(To view documents posted on this web site as PDF files or in other formats, please read our Format help page.)