Executive Summary
Americans want a health care system that works for everyone. But the reality is that the health care system that captures vast amounts of America’s resources, employs many of its talented citizens, and promises to both promote health as well as relieve the burdens of illness is failing far too many of us.
Over the past year, the number of uninsured has grown by more than one million, and tens of millions more are underinsured, and at immediate risk of financial ruin if they are seriously ill or injured. Individuals, families, employers, and every level of government are feeling the financial pressure of rising health care costs. More often than not, people do not receive the best care that science has to offer. Many are bewildered by the complexity of health care and insurance coverage. As one citizen voiced to us, you cannot “navigate the health care system without luck, a relationship, money and perseverance.”
The need for change is clear, but transforming health care so that it works for all Americans is a daunting prospect. It will involve difficult decisions about how health care is organized, delivered, and financed. Years of stalemate on health reform prompted a bipartisan call to go back to the American people, to explore their values and aspirations for the health care system, and to provide the energy needed to sustain real health reform.
The Citizens’ Health Care Working Group was established by Congress to “engage in an informed national public debate to make choices about the services they want covered, what health care coverage they want, and how they are willing to pay for coverage.”
What we heard was that many Americans believe that public policy designed to address the growing crisis in health care cannot succeed unless all Americans are able to get the health care they need, when they need it.
Public Dialogue
Following six regional hearings held in 2005 with experts, stakeholders, scholars, and public officials, the Working Group issued The Health Report to the American People, a report intended to facilitate a national dialogue on health care reform. In addition, the Working Group made the presentations from its hearings available to the public via the Internet, at www.CitizensHealthCare.gov.
The Working Group then began its conversations in communities all across America. This required an extraordinary effort to reach out to diverse communities representing a full spectrum of the American public. This also included a review and analysis of policy and research literature, national polls and surveys, and special analyses of health data; live one-on-one conversations and community meetings; expert research; and mass communications through the Internet and press. Over nearly eighteen months, the Working Group engaged thousands of Americans, including:
-
About 6,650 people attending 84 community meetings across the nation as well as meetings organized by individual Working Group Members and other organizations by the end of May, 2006, and input from over 700 people attending 14 meetings after the Interim Recommendations were published on June 2nd.
-
Over 14,000 responses to the Working Group Internet poll; and another 6,000 sets of responses to open-ended questions about health care in America
-
Over 500 descriptions of experiences with the health care system submitted via the Internet or on paper, and about 400 email letters, handwritten notes, letters, essays, and copies of reports that people sent to the Working Group.
-
About 7,300 individual email and written comments on the Working Group’s Interim Recommendations
The Working Group recognized that many people attending the meetings or providing input in writing are apt to be especially interested in health care. Because of this, the Working Group held a variety of special topic meetings, some in collaboration with partner organizations, and also worked with a range of organizations to encourage their members to complete the Working Group poll or to write in comments. Among these were meetings organized by, or with the help of, groups including local Chambers of Commerce, The National Association of Realtors, The Consolidated Tribal Health Council, a consortium of Big Ten Universities, local chapters of the League of Women Voters, professional nursing associations, organizations serving homeless persons, unemployed persons, people with disabilities, and elderly persons. Several national corporations and national labor unions encouraged members to attend meetings and provide input via the Internet, and both the Catholic Health Association and the United Church of Christ were particularly active in eliciting input to the Working Group.
The remarkable consistency of findings across many communities and between the poll data obtained through the Working Group Internet site, the University Town Hall Survey, and the community meetings provides support for the view that was heard from a significant segment of the American people. The consistency with findings from recent national polls and surveys provides even stronger support for the findings. We do not claim that we know, with complete certainty, the health care values and preferences of all Americans. Rather, we based our deliberations on a careful assessment of input from as many sources as feasible, including tens of thousands of people from all across the United States, taking into account the gaps or biases that may be reflected in the data.
What We Heard
In every venue, we heard from Americans who are deeply concerned about access to health care, and the rising costs of care and insurance. While Americans recognize that health care costs are a major problem for businesses, industry, and government as well as families, many believe that the tremendous amount of resources now being spent on health care should be enough to ensure access to quality care for everyone, if these resources were allocated more efficiently. At the same time, people consistently emphasized the importance of shared responsibility and fairness – a clear willingness to pay a fair share, to try to do a better job of taking care of themselves, and to accept limits on coverage if based on good medical evidence. Many believe that health coverage should be comprehensive enough to ensure people can get the care they need, when they need it, without having to negotiate or hurdle complicated administrative barriers. They told us they want health care to be available where people need it, in their communities. Finally, people told us that they want interactions with health providers to be based on mutual trust and respect.
The Working Group heard a variety of preferences regarding how a national system of health care should be organized -- from support for an entirely federal system with no private health insurance at all, to state-based single payer systems, to private sector participation in a system with established standards for benefits, coverage, and cost with minimum government involvement in day-to-day operations, to entirely free-market approaches. There was, however, overwhelming support for a plan that covered all Americans. In addition, there was considerable discussion at many meetings about interim reforms that could increase coverage until comprehensive changes could be made. Opinions about incremental reforms were sharply divided, and varied considerably from community to community. The overriding message, however, was consistent across every venue we explored:
Americans should have a health care system where everyone participates, regardless of their financial resources or health status, with benefits that are sufficiently comprehensive to ensure access to appropriate, high-quality care without endangering individual or family financial security.
People also conveyed a sense of urgency and wanted changes to start immediately.
Values and Principles
In developing recommendations, the Citizens’ Health Care Working Group believes that reform of the health care system should be guided by principles that reflect the values of the American people:
-
Health and health care are fundamental to the well-being and security of the American people.
-
Health care is a shared social responsibility. This is defined as, on the one hand, the nation or community’s responsibility for the health and security of its people, and on the other hand, the individual’s responsibility to be a good steward of health care resources.
-
All Americans should have access to a set of core health care services across the continuum of care that includes wellness and preventive services. This defined set of benefits should be guaranteed for all, across their lifespan, in a simple and seamless manner. These benefits should be portable and independent of health status, working status, age, income or other categorical factors that might otherwise affect health-insurance status.
-
Health care spending needs to be considered in the context of other societal needs and responsibilities. Because resources for health care spending are not unlimited, the efficient use of public and private resources is critical.
Recommendations
Based on these values and principles, the Working Group proposes six recommendations – organized into three sets – to accomplish its central goal, stated in Recommendation 1: Establish public policy that all Americans have affordable health care.
A clear majority of participants in community meetings, as well as those who responded to a variety of national polls conducted over the past few years, are in favor of a national system that provides universal coverage. However, “universal coverage” means different things to different people. The values and preferences being expressed did not lead the Working Group to conclude that there was only one particular model for ensuring that all Americans have access to high quality health care. Several approaches need to be analyzed and debated.
What is clear is that all Americans want a health care system that is easy to navigate. They want to have stable coverage when circumstances change, such as when they change jobs, get married, or move to different state. People want decisions about what is and what is not covered to be made in a participatory process that is transparent and accountable. It should draw on best practices, resulting in a clearly defined set of benefits guaranteed for all Americans. The overwhelming majority of Americans that the Working Group heard from also want health care system change to begin now. The Working Group is therefore recommending immediate action with a target of 2012 for ensuring a core set of benefits and services for all Americans.
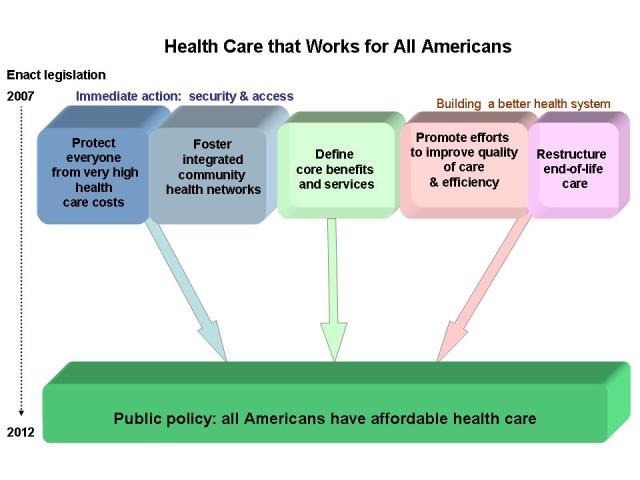
The Working Group proposes a five-year transition with the immediate first step to address serious threats to health security – very high costs, and gaps in access to basic health care, preventive services, and health education at the community level. This step combines two recommendations.
ONE: Immediate action to improve security and access
Recommendation 2 calls for creating a program that could be implemented in the relatively short term that would provide a basic level of financial protection to everyone: Guarantee financial protection against very high health care costs.
The program the Working Group is recommending would provide some level of immediate protection for everyone, and also has the potential to stabilize existing employer-based health insurance markets and expand the private individual and small group health insurance market to more Americans. More important, it will provide the foundation for providing core benefits and services to all Americans called for in Recommendation 1. This program could be structured in a number of ways, using market- based or public social insurance models.
Recommendation 3 addresses serious concerns we heard across the country related to a lack of primary-care providers; the inability to access specialty care; and, difficulties in navigating a complicated system, especially for those with chronic conditions: Foster innovative integrated community health networks.
Citizens in multiple locations spoke highly of the continuity of care and easy access to needed services they receive from comprehensive delivery systems. The goal is to help communities build programs where health care providers at the local level work together to ensure that more people can have a “medical home” and access to primary care, mental health, and dental health care, and improve the effectiveness and efficiency of health care delivery.
TWO: Define Core Benefits and Services for All Americans
Perhaps the most challenging component of the Working Group’s strategy is Recommendation 4: Defining the core benefits and services that will be assured to all Americans.
The conversations in each and every community meeting demonstrated how difficult the task of defining basic health care coverage will be for policymakers. Many people expressed concerns about what they view as the arbitrary exclusion of benefits or services from coverage. As was the case in many deliberations, the public was aware of the political challenges involved in making such decisions and the virtues of independent commissions in helping policymakers with such choices.
To define core benefits and services for all Americans, the best methods must be applied in a transparent process. Consumer participation is critical to ensuring public trust in the process and essential for ensuring that personal values and preferences are taken into consideration in coverage decisions. The group making decisions should be established as a public/private entity to insulate it from both political and financial influence. The group should be an ongoing entity with stable funding, to guarantee its independence and to assure that the benefits continue to reflect advances in medical research and practice. Evidence used to make decisions about coverage can contribute to improvements in the overall efficiency of health care delivery and help patients and providers make informed decisions. Identifying core benefits can help make all health care more effective and efficient, helping to control health care costs overall.
THREE: Build a Better Health System
A message that resonated throughout the public discourse centered on how America could do a better job with its $2 trillion a year spending on health by achieving greater efficiency and improving quality.
Recommendation 5 reflects the urgency of creating the tools and infrastructure to support a more efficient and effective health care system: Promote efforts to improve quality of care and efficiency.
Concerted efforts in some integrated health care systems have demonstrated how care can be improved and waste largely eliminated. Continuous improvement methods have reduced costs by managing chronic conditions, providing tools for informed decision-making, reducing preventable care-associated patient injuries, and designing coordinated systems of care delivery that reduce hassle and the need to redo tests and procedures. However, continuous improvement efforts rest on fundamental changes in medical practice and culture – a difficult, long-term, proposition. Widespread improvement will require a much better understanding of how to “do it better” (investment in health care delivery research), restructured training programs, significant organizational restructuring, and investment in aligned health information technologies and systems.
The federal government is a dominant purchaser of health care. It also plays a significant role in the research and evaluation of the delivery of health care services. It is well positioned to provide leadership in these areas. A variety of federal programs could be used for development, demonstration, and dissemination. Federal health programs run the full range of design possibilities, making them particularly useful for the “beta testing” of new ideas. Recommendation 5 focuses on advancing the pace of the work that needs to be done to build a health care system that works better for everyone.
Recommendation 6 focuses on an especially difficult, often expensive aspect of health care that, in many ways, reveals some of the most serious problems with our health care system: End-of-life care should be fundamentally restructured so that people of all ages have increased access to these services in the environment they choose.
Many end-of-life issues are intertwined with effectiveness, quality of care, clinical decision-making, and patient education addressed in Recommendation 5. The concerned and thoughtful attention to end-of-life issues that emerged through its public dialogue made clear to the Working Group that change is needed.
Currently, the policy development is hampered by a lack of useful information about patients’ needs and use of services. The development and use of standardized instruments for collecting demographic, epidemiological, and clinical information, careful evaluation of emerging care models, and the dissemination of best practices are all needed to improve care for the dying. The Working Group acknowledges that end-of-life issues are often difficult, painful, and complicated and thus not conducive to quick or easy fixes This recommendation seeks to better define, communicate, and make available at individual, family, community, and societal levels the support needed and wanted in one’s last days.
Public and private payers should integrate evidence-based science, expert consensus, and linguistically appropriate and culturally sensitive end-of-life care models so that health services and community-based care can better handle the clinical realities and actual needs of patients of any age and their families.
Concluding Remarks
Adopting these strategies simultaneously enables the American health care delivery and financing systems to take several important steps toward universality. It sets in motion a plan that responds to overwhelming public support for a new dynamic in American health care where everyone is protected, not just select portions of the population.
In the recommendations that follow, the Working Group acknowledges that while improvements in health care organization and delivery can yield savings over time, implementing these recommendations will likely require new resources. It has identified principles that any new funding source should meet and offers examples of options already part of the policy debate that meet these criteria.
More detailed information, including background on the state of health
care in America, analysis from the community meetings, comments and
opinions provided to the Working Group, and relevant data from national
polls and surveys, is provided in Health Care That Works for All
Americans: Dialogue With the American People and Report to
the American People (Revised 2006).
(To view documents posted on this web site as PDF files or in other formats, please read our Format help page.)