[view PDF version of this document]
In the Summer and early Fall of 2005, the Working Group held hearings in Crystal City, Virginia; Jackson, Mississippi; Salt Lake City, Utah; Houston, Texas; Boston, Massachusetts; and Portland, Oregon to learn about the nation’s health care system. At the first hearings, health policy experts provided a common foundation on topics including employer-based and other private insurance, public programs including Medicare and Medicaid, health care costs, and public and private initiatives to control costs and expand insurance coverage. At the subsequent hearings topics included: the uninsured and underserved, health care quality, geographic variation in health care utilization, health information technology, rural health issues, mental health, health care disparities, long term care, end of life care, community based care, and Oregon’s experience in public engagement on health care issues.
We also heard of many private and public programs trying to expand access to care, improve quality, and reduce costs. Some of the programs we heard about were state and local programs to expand health insurance coverage; employees and employers working together to expand access by holding costs down and getting the right care at a good price; using health care technology to reduce medical errors, monitor patient care, and choose the most appropriate care for patients; providing more information to providers and patients for making choices about health care; encouraging people to use less expensive but equally effective care such as generic drugs; adjusting payments to doctors, hospitals, and other health care providers based on the quality of care they provide; and improving people’s access to care and insurance coverage through more effective use of current programs or new programs that will allow small business and self employed individuals to obtain coverage.
Many of the programs are new, so we don’t know yet how well they will work over the long-term. And, because these programs were designed to work in particular places, we don’t know whether the programs would fit, or work successfully, in other locations or settings. However, the hearings reinforced our conclusion, as stated in the Health Report to the American People, that we need to address the entire health care system, not just specific problems in cost, quality, or access, no matter how urgent they may seem from our different perspectives. Ideally, savings gained from improving efficiency and quality in the system could be used to make other needed changes. Some of the proposed health care initiatives could help to keep the amount and type of some health care services we receive the same, while controlling costs and improving quality. But we also concluded that none of the initiatives that we reviewed could provide all the answers to our health care system’s problems. Rather, the hearings helped lay the groundwork for the search for solutions described in this report.
A complete list and brief description of the 61 presentations made by experts at these hearings is found in Appendix E.
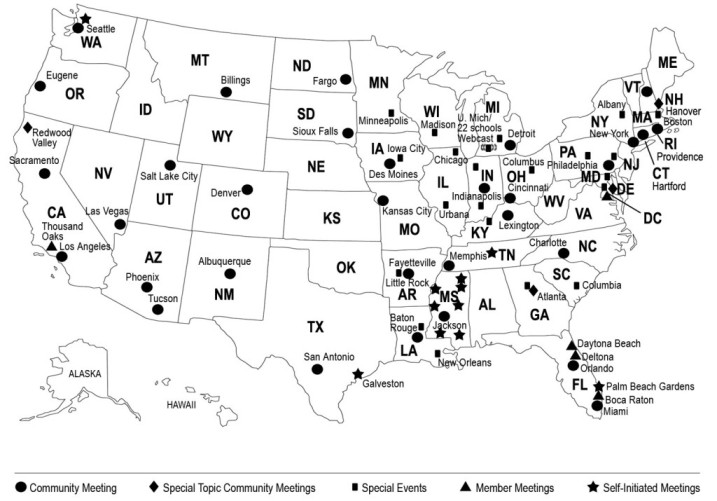
The Working Group conducted community meetings throughout the United States to hear from, and begin a dialogue with, the American people. As stated in the statute, these meetings constitute the primary source of input that the Working Group has used in developing its preliminary recommendations. In addition, however, a variety of complementary forms of input (described below) have been important. These different types of input were designed to engage a broad segment of the American public in an informed discussion, using formats that allowed both
The Working Group conducted 31 Community Meetings in 28 states between January and May 2006 (see Appendix A). These meetings ranged in size from about 35 to approximately 500 participants. At least one Working Group Member attended each meeting. Each meeting was organized using one of a set of formats designed for meetings of different lengths, but all were based on discussion of the four questions to the American people posed in the legislation. The discussion guides, as well as other background materials developed for the meetings (videos, slides, etc.) were all based on the analysis of issues confronting the American health care system presented in the Working Group’s publication, The Health Report to the American People, with some updated facts and figures. Audience generation for the community meetings consisted of outreach through both earned and paid media, involvement of national and local organizations, associations, and other groups, and the participation of various leaders and government officials at the local, state and national level. Professional meeting facilitators led the meetings.
The basic structure of the meetings involved discussion among participants sitting in small groups, and a structured process for reporting the views of the groups. At the 31 Community Meetings, electronic devices allowed individuals to provide responses to all or some of the same questions included in the poll posted on the Working Group Internet site (see Appendix C), and used in other polls and surveys. The responses to each question were then displayed on a screen, providing immediate feedback to the participants. As discussed in “The Dialogue with the American People”, there was some variation in the wording of the “standard” questions from meeting to meeting, in response to the preferences of the groups. The format therefore allowed participants to alter the discussion when they felt it was important to do so, while providing enough consistency to allow for comparisons on key issues. Attendees were also encouraged to provide written comments, and many did so. Staff of the Working Group also considered these comments in their review of the meetings.
Another important set of discussions took place at the University town hall meeting sponsored by the Big Ten Conference and the Association of Schools of Public Health, and hosted by the University of Michigan on March 22, 2006 (Appendix D). This virtual town hall provided a forum for individuals gathered at 22 separate public meetings organized by the participating universities, along with the host meeting at the University of Michigan, as well as people viewing the live webcast across the country. Interactive technology allowed various locations to call in with questions and comments, and individuals submitted their feedback about health care in America through email to be read to participants during the live event.
Still other meetings organized by individual Working Group Members and staff
in collaboration with community based health, advocacy, and business groups
provided additional insights and opportunities to hear from people with perspectives
that might not have been well represented at the other community meetings (see
below). Some of these were directly related to issues that were raised in the
hearings held by the Working Group (see Appendix E). These special meetings
included sessions focusing on mental health, health care at the end of life,
chronic illness and disability, a series of meetings in rural areas of Mississippi,
a meeting co-hosted with Native American organizations, and a meeting organized
by a national association representing realtors.
The Working Group also reviewed data from additional meetings that members as
well as other people throughout the country conducted on their own, using materials
developed by the Working Group and made available to the public in the “Community
Meeting Kit” available on the website. A listing of meetings that have provided
data to the Working Group is included at the end of this section. Other organizations
have also provided us with information. Among these are: The National Health
Care for the Homeless Council (NHCHC), which conducted a nationwide outreach
effort to gather the input of homeless persons; data from the responses of 446
homeless persons in 12 cities were provided to the Working Group. The United
Church of Christ provided us with about 1,500 hand-written responses from people
in about 10 percent of its 5,700 churches across the country to the open-ended
questions posted on our Internet site. Additionally, the Area Agency on Aging
in Florida provided about 50 poll responses from seniors in Florida. The Catholic
Health Association also provided over 1,000 poll responses from its members.
The Working Group solicited input from people across the country via the internet, at www.citizenshealthcare.gov, and by mail.
The Working Group Public Comment Center on its website solicited both structured and unstructured comments from the public.
Written input, including paper versions of the internet poll as well as written responses to the open-ended questions that were mailed to the Working Group, were also coded and analyzed using the same protocols as the electronic data submitted over the Internet.
Methods
The Working Group reviewed summaries of all the sources described above. The Community Meetings were considered, for analytical purposes, as case studies. In addition to the data on demographics and the votes recorded at each meeting, staff reviewed background information on each location and, in the course of planning each meeting, obtained a great deal of information on the health care, resources, and policy issues in each community. Senior staff members who attended the meetings used a structured format when preparing the meeting reports. The individual reports, including the data recorded at each meeting, are being made available to the public on www.citizenshealthcare.gov. The Working Group compared data across meetings only when it was truly comparable, that is, questions were asked in the same context during the meetings, in the same form. (See Appendix B for more information.)
Data from open-ended and poll responses were coded by staff and analyzed using standard statistical software. The Working Group reviewed summary data, as well as the results of analyses possible differences in response patterns related to demographic differences. The Working Group also reviewed data from relevant national polls and surveys.
People attending the Working Group Community Meetings or providing input in writing are more likely than others to be especially interested in health care, either because they, or their family members, have had concerns about their health care or insurance coverage, or because they work in the health care field. The people we heard from were, on average, more likely to be female and in or on the edges of the Baby Boom generation (age 45-64), and the proportion having bachelor degrees or advanced graduate degrees was much higher than in the population as a whole. And, while participation in Community Meetings by minority group members was fairly close to national percentages, representation of people who identified themselves as Latino or as African American among those submitting comments or poll data was lower. The proportion of people who were not covered by any form of health insurance, and the proportion receiving benefits through Medicaid, was also lower than the nation as a whole. Some of these limitations were addressed by holding meetings specifically designed to reach underrepresented populations (see above). And, as noted above, analysis of the data was performed to assess the extent to which demographic factors may have accounted for some of the findings.
A more serious issue is the inability to ensure that people providing input represent the full spectrum of views of all Americans, given that people who are sufficiently interested or motivated to provide input on health care and policy issues may not be typical of the population as a whole. To some extent, consistency of findings across many communities and between the poll data obtained through both the Working Group Internet and the University town hall meeting provides support for the view that we have heard from a significant segment of the American people. The consistency between findings from recent national polls and surveys provides even stronger support for the findings. However, the meetings, as well as the www.citizenshealthcare.gov data were designed to offer information to help frame discussion and responses to questions, whereas national polls and surveys generally do not serve this purpose. Therefore the responses we have analyzed are not exactly comparable to other national poll data, even when the same, or very similar, questions are asked. Consequently, we do not claim that we know, with great certainty, the values and preferences of all Americans. Rather, we are basing our recommendations on a careful assessment of input from as many sources as feasible, from thousands of people from all across the United States, taking into account the gaps or biases that may be reflected in the data to the best of our ability.
| Kansas City, MO | January 17, 2006 |
| Orlando, FL |
January 24, 2006 |
| Baton Rouge, LA | January 26, 2006 |
| Memphis, TN |
February 11, 2006 |
| Charlotte, NC | February 18, 2006 |
| Jackson, MS | February 22, 2006 |
| Seattle, WA | February 25, 2006 |
| Denver, CO | February 27, 2006 |
| Los Angeles, CA |
March 4, 2006 |
| Providence, RI | March 6, 2006 |
| Miami, FL | March 9, 2006 |
| Indianapolis, IN | March 11, 2006 |
| Detroit, MI |
March 18, 2006 |
| Albuquerque, NM | March 20, 2006 |
| Phoenix, AZ | March 25, 2006 |
| Hartford, CT |
April 6, 2006 |
| Des Moines, IA | April 8, 2006 |
| Philadelphia, PA | April 10, 2006 |
| Las Vegas, NV | April 11, 2006 |
| Eugene, OR | April 18, 2006 |
| Sacramento, CA |
April 19, 2006 |
| San Antonio, TX | April 19, 2006 |
| Billings, MT | April 21, 2006 |
| Fargo, ND | April 22, 2006 |
| New York, NY |
April 22, 2006 |
| Lexington, KY | April 25, 2006 |
| Cincinnati, OH | April 29, 2006 |
| Little Rock, AR | April 29, 2006 |
| Tucson, AZ | May 4, 2006 |
| Sioux Falls, SD | May 6, 2006 |
| Salt Lake City, UT | May 6, 2006 |
| Hanover, NH | Last Days | March 31, 2006 |
| Redwood Valley, CA | Native Americans | April 20, 2006 |
| Washington, DC | National Association of Realtors | May 16, 2006 |
| Atlanta, GA | Mental Health | May 22, 2006 |
Meetings Organized by Individual Members
| Washington, DC | Ascension Health CEOs | December 5, 2005 |
| Daytona Beach, FL | Bethune-Cookman College | March 26, 2006 |
| Deltona, FL | Florida CHAIN (Community Health Action Information Network) and MS-keteers Multiple Sclerosis Support Group | May 6, 2006 |
| Palm Beach Gardens, FL | Area Agency on Aging | May 10, 2006 |
| Boca Raton, FL | Area Agency on Aging | May 11, 2006 |
| Lake Worth, FL | Area Agency on Aging | May 12, 2006 |
| Thousand Oaks, CA | City of Thousand Oaks Conejo Recreation and Park District | May 18, 2006 |
National Webcast, March 22, 2006
| Participating Institutions# | |
| Boston University | Boston, MA |
| Drexel University | Philadelphia, PA |
| Emory University | Atlanta, GA |
| George Washington University | Washington, DC |
| Indiana University | Indianapolis, IN |
| Johns Hopkins University | Baltimore, MD |
| Louisiana State University | Baton Rouge, LA |
| Michigan State University | East Lansing, MI |
| Northwestern University | Evanston, IL |
| Ohio State University | Columbus, OH |
| Penn State University | Harrisburg, PA |
| Purdue University | West Lafayette, IN |
| Tulane University | New Orleans, LA |
| University at Albany | Albany, NY |
| University of Arkansas | Fayetteville, AR |
| University of Illinois | Urbana, IL |
| University of Iowa | Iowa City, IA |
| University of Louisville | Louisville, KY |
| University of Michigan (Host) | Ann Arbor, MI |
| University of Minnesota | Minneapolis, MN |
| University of South Carolina | Columbia, SC |
| University of Wisconsin | Madison, WI |
# Not all meetings took place at main campuses.
Self-Initiated Meetings
Crossville, TN |
The Learning Community | January-March, 2006 |
| Starkville, MS | MSU Extension | March 21, 2006* |
| Verona, MS | MSU Extension | March 27, 2006* |
| Wesson, MS | MSU Extension | March 29, 2006* |
| Hattiesburg, MS | MSU Extension | March 30, 2006* |
| Clarksdale, MS | MSU Extension | April 11, 2006* |
| Palm Beach Gardens, FL |
Human Resource Association of Palm Beach County | April 11, 2006 |
| Greenville, MS | MSU Extension | April 18, 2006* |
| Newton, MS | MSU Extension | April 20, 2006* |
| Eau Claire, WI | Chippewa Valley Technical College | April 29, 2006 |
| Seattle, WA | Association of Advanced Practice Psychiatric Nursing | April 29, 2006 |
| Galveston, TX | Center to Eliminate Health Disparities, University of Texas Medical Branch | May 1-3, 2006 |
| McKeesport, PA | Mon Valley Unemployed Committee | May 11, 2006 |
* Held under the auspices of the Mississippi State University Extension Service.