
An Invitation to Make Health Care Work for all Americans
See this document in print-ready PDF format (color PDF; black and white PDF)
(To view documents posted on this web site as PDF files or in other
formats, please read our Format help
page.)
You're Invited...
To become a part of an historic discussion taking place right now across America where citizens like you get to tell the policymakers in Washington what you like and dont like about our nations health care system, and what tough choices our country should make to turn it into one that works for all Americans.
Under a new federal law, the public involvement that we hope you will be part of must be followed up promptly with Congressional hearings and action on what you and other Americans want the health care system to be.
Thats why this isnt just another public opinion poll. Its not another one of those endless discussions that never seem to change anything. It is a chance for every citizen to shape national policy: to get the facts, weigh the tradeoffs, and tell the President and Congress exactly how you want your health care system to change.
And you need to take part:
- Because as a citizen, you care about your health and that of your family, friends, neighbors, and community.
- Because as a consumer, you care about having access to affordable care thats high quality.
- Because as a taxpayer, you care about keeping the cost of care under control, and you want it delivered as efficiently and as waste-free as possible.
This is a discussion that cant happen without you. Neither will the Congressional action. In 2003, Congress passed a law saying that In order to improve the health care system, the American public must engage in an informed national public debate to make choices about the services they want covered, what health care coverage they want, and how they are willing to pay for coverage. This is your chance to create a citizens roadmap to health care that works for all Americans.
To get that discussion off the ground, Congress created a Citizens Health Care Working Group, whose job it is to help you understand the facts and issues and then be heard.
And your voice does matter. Your opinions will help form a citizens action plan for the President and Congress to consider as they work to make health care work for all Americans.
So please join in!
Start by reading this booklet and getting comfortable with the key
facts and issues. (Much more free information such as a detailed report,
video, and slideshow is available online at www.citizenshealthcare.gov).
Later well tell you how to make your voice heard.
Cost, Quality and Access
Our health care system is complicated, but there are three basic issues that we need to talk about: Cost. Quality. Access.
- Cost is what is paid for health care. We ALL pay one way or the other, in employer or employee contributions, in taxes, in insurance premiums, or directly out of pocket.
- Quality refers to the kind of care you get the right care at the right time, safe care, respectful of your wishes in a manner thats right for you, so that your health and quality of life improve.
- Access involves whether care is available and affordable. Insurance coverage, whether its private insurance or a public program like Medicare or Medicaid helps to make sure that we can get care when we seek it.
In Our Health Care System, Everything is Related to Everything Else
Cost, quality, and access are not independent of each other. Our health care system is a lot like our natural environment an ecosystem, in which any significant change in one area has ripple effects throughout the others.
|
I was an elementary science teacher. I ate right, exercised regularly,
and was rarely ill. I had only fleeting contact with the health
care system. But then I got sick. I was always tired no matter how
much sleep I got. My vision became blurry, and I had difficulty
hearing sometimes. Eventually I was diagnosed with multiple sclerosis,
a chronic neurological disease. - Montye Colan Citizens' Health Care Working Group member Ormond Beach, FL |
Cost, quality, and access can support each other. For example, better treatment of illness earlier can prevent serious complications that could land people in the hospital and cost a lot of money.
Sometimes, increasing costs keep people from getting the care they need. For instance, higher health insurance costs can lead employers to cut down on the amount of insurance coverage they offer their employees. This can lead to more people without insurance or with inadequate benefits and with less access to care. Poor quality care with medical errors can cause problems that are very expensive to treat. Any change we make that affects costs, access to care, or quality may affect this system in ways that are difficult to predict.
Thats one more reason why some of the choices we have to make are so tough. There are trade-offs to weigh in every decision we make. Piecemeal changes on their own have not been enough to address the complex web of problems that affect the health care system. So we need to work on the whole system all at once. And we need to find win-win solutions things that improve quality and access while reducing costs. That will take time and a lot of hard work.
So we begin by asking: What are the facts? And what are the issues?
Cost: How Much Do We Spend, and For What?
Key Facts about the Cost of Health Care in America:
1. We pay for health care through both private funds and public dollars. Either way, it comes out of our own pockets.
Private spending is what we pay for health care, either through insurance or directly with our own money.
| My husband had some complications with his back surgery and wound up on a respirator in the intensive care unit for five days and in a neuro-acute unit for four more days. Even though he and I both had insurance, the 20 percent of the bill that I would have had to pay was $80,000. Christine Wright Citizens Health Care Working Group member Sioux Falls, SD |
- Public spending for health care comes from tax dollars that federal, state, and local governments use to pay for programs like Medicare and Medicaid. Today, Medicare and Medicaid spending account for almost one out of every five dollars the federal government spends. Thats likely to become one out of every three dollars by 2040.
- Government also helps to pay for health care through tax breaks for employees whose employers offer health benefits.
2. Costs are rising sharply.
- Back in 1960, we spent about a nickel out of every dollar we earned on health care in the United States. That was about the same amount we spent on education. Today, the percent going to health care has tripled, while what we spend on education hasnt even doubled.
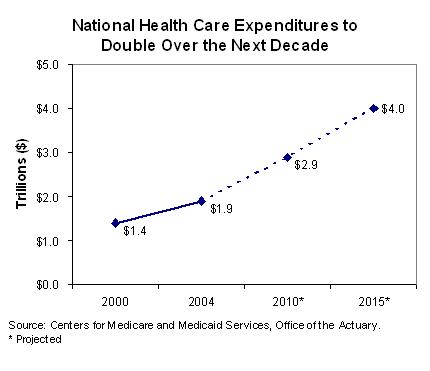
- In 2004, Americas total health care bill came to $1.8 trillion. If you added up every dollar earned by every American worker in the first two months of the year, the total would be this amount.
- For each person, we spent about $6,400 on health care in 2004. In ten years, this amount is expected to rise to $11,000.
- Part of the cost of care is the money spent on medical research. It underpins significant advances in the care we receive. As a result, the U.S. is the leader in the development of new technologies and remedies, especially drugs, which greatly improve our lives.
3. Higher costs can result in less coverage and less care.
- Higher health care costs mean insurers have to charge higher premiums. This makes employers less likely to offer coverage that employees can afford.
- In 2004, about one in 20 Americans reported that costs prevented them from obtaining needed care.
National Health Expenditures to Double Over the Next Decade
4. Our need for health care and spending varies a lot and changes over the course of our lives.
- In any given year, close to 50 percent of all health care spending pays for the care received by only 5 percent of the population.
- Health care for people with chronic diseases accounts for 75 percent of our total health care costs. Managing these illnesses can be expensive. For example, in 2002, people with diabetes spent, on average, $13,243 on health care bills.
- Other things, such as serious illnesses, accidents, or premature births, can be very expensive. Hospital charges alone can top $100,000 for these cases.
- Health care needs tend to increase over time. On average, only about one-fifth of all the money that will ever be spent on our health care is for health care we use in the first half of our lives. But half of all the money spent on our health care will be for care we get after we turn age 65. On average, health care costs for people ages 76 to 84 are about $8,000 every year. This is almost eight times as much as for children between 1 and 5 years old.
5. Waste and inefficiency also contribute to higher costs.
- We pay for health care in a very complicated way. Complex billing and paperwork may result in relatively high administrative costs in the United States and can be frustrating for patients, doctors, hospitals, and insurance companies.
Quality: Are We Getting Our Moneys Worth?
Key Facts about the Quality of Health Care in America:
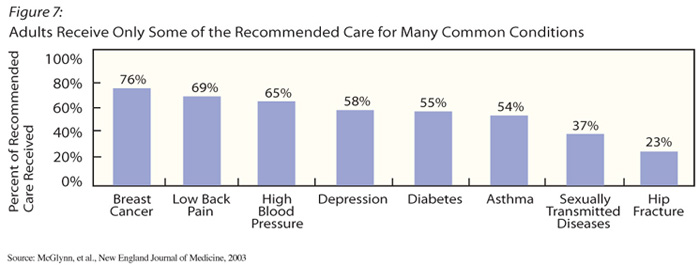
1. Despite all the money we spend, people often do not get the care they need.
- Overall, adults get only 55 percent of the recommended care for many common conditions.
2. Despite spending more per person on health care than other developed countries, our results are not consistently better and are sometimes worse.
- For example, the United States has seen an increase in the death rate from asthma in recent years, while death rates for asthma have declined in Canada, the United Kingdom, Australia, and New Zealand.
3. The quality of our health care often depends on where we live and who we are.
- There is consistent evidence of a difference in the availability and quality of care related to race, ethnicity, and income.
Adults Receive Only Some of the Recommended Care for Many
Common Conditions
- In fact, African Americans, Asian Americans, American Indians, and Alaskan Natives and particularly Hispanic Americans generally receive poorer quality of care and have poorer access to care than white, non-Hispanic Americans.
- People with incomes below the poverty level report poorer access to care and have more problems with the quality of their care than people with higher incomes.
4. Poor quality can consist of either too little or too much care.
- Certain services like vaccines, colonoscopies, complete preventive care for diabetes, treatment for depression, and medicines to prevent additional heart attacks are all underused. That means that not everyone who should receive services does.
- On the other hand, some health care services are used too much. Some surgeries are not necessary and do not help people. Antibiotics are not effective in treating colds and other viruses, but they are still being prescribed for treating these conditions.
- The amount of health care services that people use varies a lot across different parts of the United States, and can be affected by the number and types of health care providers where they live.
| I have five
kids and five grandkids. And what was normal for me when I entered
the workforce in the 60s was, you took health care for granted
and you expected decent health care coverage. The same expectation
is not there for them as we go into the future. Joe Hansen Citizens Health Care Working Group member Washington, D.C. |
5. Medical errors are a particularly harmful form of poor quality.
- An estimated 44,000 to 98,000 Americans die every year as a result of medical errors. This is more than the number of people who die from car accidents, breast cancer, or AIDS alone.
- Its believed that medical errors occur in 2 to 4 percent of hospitalizations.
6. Our health habits affect our health and the quality of our lives.
- About 40 percent of American adults are not physically active, and nearly two-thirds are overweight or obese. While not everyone can be physically active, many people can reduce their risk for heart disease, diabetes, and some types of cancer by losing weight and exercising more.
- Many people begin smoking despite its serious harmful effects.
Access: Who is Getting Care And Who Isnt?
Key Facts about Access to Health Care in America:
1. Almost 46 million Americans have no health insurance.
- The uninsured are not necessarily poor. Most are members of working families, and most have incomes above the poverty line. Even so, many people cant afford to buy health insurance. Some uninsured people who could afford to buy it choose not to do so.
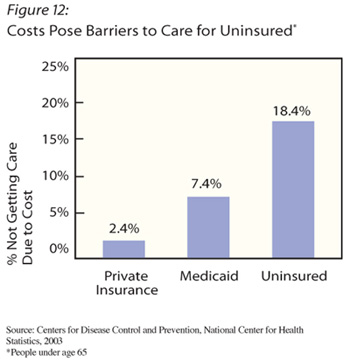
2. Those without coverage often dont get the care they need.
- Uninsured Americans are nearly eight times more likely than people who have insurance to skip health care because they cant afford it. And, this can lead to more serious illnesses that need to be treated in an emergency room or the hospital. These services cost much more than it would cost to treat the original problem. About half of uninsured adults with chronic health conditions go without recommended health care or medicines because of cost.
Costs Pose Barriers to the Uninsured
3. The most important source of health insurance for workers is employer-sponsored group coverage. But this is getting less common and more costly.
- Seven out of 10 Americans who have some form of health insurance coverage get it through an employer.
- The percent of people covered by employer-sponsored health insurance declined from 64 percent in 1999 to 60 percent in 2004.
- In 2004, just about all large companies offered their employees health insurance. But only half of the smallest companies (with fewer than 10 employees) did.
- Employers that do offer coverage are paying a lot more for it than before. They are also asking employees to pay more as well.
- Sometimes when Americans need coverage the most, they dont have it. This can happen because a severe illness may force them to quit work, lose insurance and the income that allows them to afford care.
- Medicaid programs vary from state to state. Low income people who qualify for assistance with Medicaid in one state may not qualify for benefits in another.
| When I was
chief resident in the 1960s, one night I lost 11 babies, and I lost
them to conditions that could have been prevented. In those days,
babies died because of infectious diseases and severe dehydration.
We had antibiotics back then, and we knew how to treat those conditions,
but in many of the communities they didnt apply the knowledge and
the technology that was available to them. Aaron Shirley Citizens Health Care Working Group member Jackson, MS |
4. Some areas of the United States do not have enough health care providers to serve everyones needs.
- The availability of services varies a great deal across the country. It is different among the states, between urban and rural areas, and from one community to another.
- More than 10 percent of Americans report not having a regular place to go when they need health care.
- Even when care is available, people can have problems getting through the health care system. For example, communication problems can make it hard to get the care you need.
Reforming Our Health Care System Is a Huge Challenge That Requires New Thinking and Creative Solutions
Many of you may know from first-hand experience what we have been talking about a health care system troubled by sharply rising costs, unreliable quality, and, for some people, poor access to care. Many people either have no health insurance, or they do not have enough insurance coverage. These problems are complicated and they affect each other.
Lots of new ideas are being explored by governments, businesses, and others. Examples include:
- Creating new state and local programs that expand insurance coverage and at the same time control costs and improve quality and access to care.
- Having employers and employees work together to expand access by holding costs down and getting the right care at a good price.
- Using new health information technology. The goal is to provide more information to providers and patients, improve quality, reduce medical errors, and reduce waste.
- Encouraging people to use less expensive, yet equally effective health care options. For example, people can often use generic drugs instead of more expensive brand-name medications.
- Providing more information to doctors, nurses, hospitals, insurance companies, employers, and consumers about higher quality, more efficient care. One way is to use a type of report card to rate the care provided by different types of health plans, hospitals, nursing homes, etc.
- Adjusting payments to doctors, hospitals, or other health care providers based on the quality of care they provide.
- Improving peoples access to care and insurance coverage through a more effective use of current public programs, such as Medicaid, or new programs that will allow more employers to offer coverage.
While some of these ideas may appear promising, not all are being used widely. Some need careful evaluation. Few of them have been easy to do. Some will prove themselves, but others just wont pan out in our complex health care system. We need lots of ideas. We still have some hard work cut out for ourselves.
Now its time to hear from you. You can help shape our health care system in the future and, hopefully, allow us to create one that works for all Americans.
We need to know about your concerns. We also need your ideas about where we go from here. Let us know what you think.
- What concerns you most about the health care system in America today?
- What health care benefits and services should be provided?
- How should health care be delivered?
- How should it be paid for?
- What have you seen in Americas health care system that works well?
- What trade-offs should the American public be willing to make in either benefits or financing to ensure access to affordable, high-quality health care coverage and services?
- What is your single most important recommendation to make to improve health care for all Americans?
These are just some of the questions that we need to answer. Well be formulating others as we grapple with problems and solutions.
So heres what to do next:
- Find out more about health care. Keep this booklet handy, so you can refer back to the key facts and issues. Learn more from the free information a detailed report and slideshow available online at www.citizenshealthcare.gov.
- Tell us what you think about what works and what does not.
| Go online to www.citizenshealthcare.gov E-mail us at citizenshealth@ahrq.gov Write to us at Citizens Health Care Working Group; 7201 Wisconsin Ave., Suite 575; Bethesda, MD 20814 |
- If possible, participate in community meetings that we will be holding around the country. (Go online to Community Meetings at www.citizenshealthcare.gov to find one near you).
- Once we hear from you and other citizens, we will be placing recommendations on the www.citizenshealthcare.gov Web site for you to review.
- And finally please urge friends, family members, colleagues, and neighbors to participate in this important movement. Get them involved in making health care work for all Americans. This is a unique opportunity dont miss it. Learn, discuss, and take action.
Citizens' Health Care Working Group
Chair |
|
| Randall L. Johnson Naperville, IL |
|
Members |
|
| Frank J. Baumeister, Jr. Portland, OR Dorothy A. Bazos Concord, NH Montye S. Conlan Ormond Beach, FL Richard G. Frank Boston, MA Joseph T. Hansen Rockville, MD Therese A. Hughes Newbury Park, CA Brent C. James Salt Lake City, UT |
Catherine G. McLaughlin Ann Arbor, MI Patricia A. Maryland Carmel, IN Rosario Perez San Antonio, TX Aaron Shirley Jackson, MS Deborah R. Stehr Lake View, IA Christine L. Wright Sioux Falls, SD |